A DUTY TO DIFFERENTIALLY DIAGNOSE :The Substance Behind the Assertion the President Has a Serious Psychiatric Condition

Vincent Greenwood, Ph.D., Founder, DutyToInform.org
Preface
On January 2, 2020, l was acclimating myself to the office after a ten-day holiday break. I oversee a small psychotherapy practice in Washington D.C. and l was hoping to ease back into the work, to hopefully have one of those days that is absent of any heavy lifting. Alas, l met with two separate clients who were in a great deal of anguish. One expressed herself with a set jaw, biting of her lip, mournful shaking of her head and watery eyes; the other with retching sobs and, at one point, slamming the arm of her chair with her fist.
It’s a therapy office, so displays of intense feeling are not exactly “stop the presses” happenings. But the similarity of the distress of the two women was striking. For each one, turning the calendar year to 2020 was what had shaken them. The advent of the New Year had the identical meaning for each of them: the election year was upon us and the stakes were existential-level profound.
Their anguish expressed more than “this is the most important election of our lifetime.” More like something precious and vital to their core was under siege. More like one of their children had been kidnapped, was being held for ransom, and it was unclear how it would all unfold. Not a child in their case, but something elemental, hard to put into words… the soul of their country?
l would not describe either of these women as “emotional.” Both are accomplished and sober-minded. I knew both would be extending themselves for the election.
I want to thank them. l had been working pretty steadily on this essay through the Fall of 2019. But after the sessions with them, l redoubled my effort and my focus geared up a level. Because implicit in their pain was a directive: “the clock is ticking…time has passed for effing around.”
A DUTY TO DIFFERENTIALLY DIAGNOSE
Thesis: The 45th President of the United States has a disorder that conveys danger to all those in his orbit. It is an affliction for which — once you learn of its essential characteristics — you would take a bullet to prevent your child from having. There is no cure for this disorder. Nor do there appear to be any effective measures to curb it. The best we might do is diagnose the disorder and warn others.
The purpose of this essay is twofold: to validate the above thesis and then to explain why this article will be ignored.
I: The Validity Underpinning the Diagnosis of The President
1
In the film, Minority Report, a science fiction movie directed by Stephen Spielberg that takes place in 2054, the Chief of Police in Washington D.C., played by a brooding Tom Cruise, is empowered to arrest individuals for murder before they commit their crime. He has been provided with this authority because there are expert visionaries (three to be exact), called Pre-Cognitives, whose prophesies of future serious crimes are never wrong.
These Pre-Cogs live in a sterile laboratory, in tanks where they are kept suspended in a twilight-like coma. They are digitally force-fed the neural circuitry of all those living in the Washington D.C. metro area and are linked up to some type of wetware/hardware interface that enables them to periodically emit the name of a potential perpetrator, who is then immediately arrested. The outcome? The murder rate in D.C. drops to zero.
The clairvoyant skills of the Pre-Cogs are never explained. They are a central plot device, a MacGuffin, to pose interesting philosophical questions that hover above the action. Questions such as, “do we have agency over our impulses and behavior, or are they determined by forces beyond our control” (the venerable free will vs. determinism debate)? Also, “what is our moral duty as a society if we had the power to predict that, some among us, are destined to inflict serious harm on our fellow citizens?” “How do we balance the civil liberties of a potential perpetrator with the safety of the community?”
Minority Report, at the outset, sets the table clearly on the side of determinism and the protection of society at the expense of individual liberty. But then, of course, complications emerge, and mayhem ensues. The film, in my opinion, devolves into a techno-crime chase thriller, with a kind of/sort of carveout that promotes the values of free will and civil liberty.
Perhaps, l shouldn’t be so harsh. After all, it’s a two-hour movie and it’s commendable to just raise thorny philosophical issues and unrealistic to expect elegant resolutions. And its science fiction, which takes place in a future world, where we can precisely predict dangerousness before it occurs. In our contemporary world, weighing the rights of the potentially dangerous seems fanciful, the stuff of fiction; or academic, the stuff of law review articles.
To truly grapple with the predicament of how to deal with someone destined to visit harm on an individual, or a community, or the world stage, we would first need a Pre-Cog, someone or some program that could discern …what? Our neural circuitry? The darkest parts of our personality? Discern the key characteristics of a potential predator that would validate the prediction of harm. But, of course, we don’t have any such Pre-Cogs in our contemporary world. Or do we?
To predict a particular person will commit a murder at a particular time and place would be a superpower at the current moment. It is beyond our reach. However, to predict that a particular person, if he suffers from a certain condition (to be described shortly), is destined to inflict significant harm and mayhem on many that cross his path, is currently possible. The ability to make that prediction flows from a legitimate act of clinical diagnosis, whose validity has been established through extensive scientific efforts.
Indeed, we can make the above prediction of dangerousness, asserted in the thesis offered at the beginning of this essay, with confidence. To explain why, we must take a brief journey through the history of the scientific study of psychological disorders.
2
It’s a brief history. It wasn’t until 1844 that psychiatry was even recognized as a medical specialty in the United States. Alas, over the subsequent 100 years, that recognition did not spur significant advances in our understanding of mental disorders. Oh, there were plenty of pioneering clinicians and researchers during this period. However, their findings and insights were destined to mostly die on the vine.
Why? Because during this time there was no formal system of classification of mental disorders and therefore no basis for making a diagnosis that possessed reliability. Reliability has a precise (psychometric is the scientific term of art) and crucial meaning in the scientific enterprise of making a clinical diagnosis. Reliability is established when clinicians and scientists, in different locations, can be confident that the patients they are diagnosing and the subjects they are selecting for research are taxonomically (scientific jargon that means descriptively) similar.
A doctor in Des Moines might come up with a useful treatment for a patient he diagnoses as depressed. But this may not be helpful to a psychiatrist in Atlanta since his diagnosis of depression is likely somewhat different. As long as diagnostic judgements were the provenance of individual clinicians or in-house products of universities and medical schools, there was no way to build upon one another’s findings. Unreliability in diagnosis tethered any breakthroughs in the understanding or treatment of mental disorders to the particular patients that benefited from those breakthroughs. Without a system of reliable diagnosis, any such breakthroughs could not be generalized to larger patient populations.
The first step in trying to achieve reliability in diagnosis of psychological disorders was to have an agreed-upon, unified system of classification of disorders. This precondition was finally met in 1952 with the publication of the first edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-I) by the American Psychiatric Association. The DSM-I was a good faith effort by leaders in the field. It contained 102 diagnoses. However, the criteria for each diagnosis were not very specific or operational. Furthermore, many of the criteria were linked to psychoanalytic theory which possessed dubious scientific validity. The DSM-II, which was published in 1968, expanded the number of diagnoses to 182 and displayed more refined criteria, but still failed to generate adequate inter-rater diagnostic agreement ratings (the standard way to establish reliability). Until clinicians and researchers could reliably make the same diagnosis, the field was stuck.
A turning point came in 1980 with the publication of the third edition of the DSM. The development of DSM-III, along with the advancement of psychometrically sound checklists
for quantitative assessment of psychological disorders, represented a paradigm shift in the art of clinical diagnosis.
The key instrumental change in DSM-III and such checklists was the development of more specific, concrete and operational criteria for each disorder. Perhaps most critically, the criteria were based on empirical research rather than theory. There was a particular emphasis on criteria that incorporated research on the course and outcome of particular disorders. There was also an effort to develop exclusion criteria i.e., characteristics that would rule out a patient for a particular diagnosis. With these refinements in the criteria, sufficient reliability was finally achieved.
With reliability established, this meant that research findings generated in London on a particular diagnostic group could be added to findings generated in Baltimore on the same diagnostic group. With reliability tucked away in their holster, researchers could now focus on the second and most critical psychometric property of clinical diagnosis: validity. The scientific definition of validity is rather recursive. Validity refers to the effectiveness of efforts to measure what it sets out to (e.g., a particular psychological disorder). Perhaps an example would help clarify. Bipolar Disorder and Major Depression share some of the same symptoms and can look similar on the surface. But mounds of research have demonstrated they are, in fact, two differentiated, coherent syndromes, each with their distinguishing signs, distinct course, and different treatment parameters.
Research, not theory, established this demarcation of these two mood disorders. Research, by identifying the meaningful constituent elements of each disorder, enables us to assert that there are two coherent syndromes for which we now have a great deal of understanding. This is what the scientific process of validity provides. It puts meat on the diagnostic bones of a disorder. And, of course, further research efforts to identify additional constituent elements will only deepen our knowledge of the disorder.
What are the kinds of things researchers focus on to establish validity of a diagnosis or checklist? Once reliability is established, a researcher could theoretically investigate any facet of a disorder. However, there has been a consensus on what to study: a five-pronged validation model that focuses on the following domains: (1) identifying the key, distinguishing clinical characteristics of the disorder; (2) pinpointing exclusionary characteristics that differentiate the disorder from other disorders; (3) family studies, with a particular emphasis on measuring the heritability for the disorder; (4) laboratory data (e.g. brain imaging, psychological testing); and (5) follow-up studies to assess diagnostic stability, and the course and response to treatment of the particular disorder.
Execution of studies in the above domains provides breadth and depth to the validity of a diagnostic category. If a particular patient meets the specific and empirically derived criteria for a certain disorder, then the diagnostician has the authority to “say a lot more” about the patient.
How much more?
3
A man in his early 60’s feels increasingly fatigued over the course of a few weeks. He tries to brush it off until one night he notices he is gasping for breath as he climbs the stairs to his bedroom. He calls his doctor the next day. The doctor instructs him to report to the lab the next morning to produce blood and urine samples and schedules an office visit for the day after that.
When he arrives for his appointment, he is immediately escorted to the doctor’s office. This unusual efficiency tweaks his anxiety. The doctor gets right to it. His white blood cell (WBC) count was abnormally high, close to 100,000 whereas the norm is closer to 7,000. The count is so high it effectively rules out the diagnosis of an infection or some other relatively benign or acute condition. He is told he has leukemia (from the Greek, leukos= white, haima= blood, and ia= condition), a blood cancer.
The doctor informs him he has already sent the blood test results to a hematopathologist. As he pulls out a white board and draws some figures on it, the doctor explains there are different types of leukemia. The hematopathologist examined his blood microscopically and saw there were circulating leukemia blasts, immature blood cells, produced by the bone marrow, that were crowding out his healthy blood cells. The doctor points to an oval figure on the white board that portrays some reddish, linear structures within the blast. These structures, called Auer rods, indicate a myeloid malignancy. His formal diagnosis is Acute Myeloid Leukemia (AML). This is not good news. Of the different types of leukemia, this is one of the least favorable. If left untreated, the disease will be fatal, possibly within weeks. He will have to undergo aggressive chemotherapy immediately. There is a 50% chance that this treatment will result in a remission, in which case he may recapture a decent quality of life. However, it is a relapsing condition which will require constant monitoring and future episodes of treatment. The doctor doesn’t tell him, but he will learn soon enough that the survival rate for someone his age, five years out from the time he receives the diagnosis, is only 4%.
The purpose of this vignette is not to educate you about leukemia, but to underscore the power and the utility of clinical diagnosis. Over the course of a few minutes, this man learns of his diagnosis and his life has changed dramatically. The ramifications — the possibilities and limits of treatment, to his sense of self, to his loved ones and colleagues, to how he will live his life — cannot be overstated.
It is tough news, this fateful diagnosis. Diagnosis is now his destiny.
But it is surely better to receive this diagnosis than remain in the dark. Now he is privy to a wealth of information, and he and his loved ones can make informed decisions about the challenges that lay ahead.
The hematopathologist here has functioned as a Pre-Cog. Because of her training and knowledge of her specialty, she has pulled back the veil and depicted this man’s future. We don’t think of her as a science fiction character, as possessing a superpower. Indeed, across the globe, there are millions of professionals in their fields of expertise who have a similar prowess. ln the modern world that can seem ordinary. But it is not. To know a great deal more about a person because you have accurately diagnosed their condition is a modern, hard-earned capacity that is only a bit shy of a superpower.
To the question, “how much more can you say about a person after you have made a reliable and valid diagnosis?” There is a simple and direct answer: as much as the accumulated findings for that disorder (or checklist) provide. With significant research comes significant authority. Indeed, when there is that sturdy empirical foundation, laid down study by study, the diagnostician of psychological disorders can speak with the equal authority of the diagnostician of blood disorders. Can speak with the authority that is just short of a superpower. Can speak as if a Pre-Cog from the world of science fiction.
With sufficient data, can speak with authority to the mental health of the President.
4
I appreciate your forbearance in making it through the history of the evolution of the statistical constructs of reliability and validity. The thesis regarding the dangerousness of the President rests on your appreciation of the informational power associated with our ability to make a reliable and valid diagnosis.
l am now going to introduce a checklist for a certain personality disorder. It was one of the first measures devised to capture this psychological disorder. It has achieved solid reliability (.89 inter-rater reliability ratings for those of you with a statistical background) and validity metrics. Because it was one of the first diagnostic instruments to develop this psychometric authority, it became the gold standard for investigating this condition, spawning over 3300 studies to date. All of the knowledge generated by these studies makes this one of the most researched and well understood psychological disorders.
The checklist, of course, has specific and operationalized criteria. If you are administered this checklist by a trained professional and reach a certain threshold of these criteria, you warrant a diagnosis of the disorder. You are then part of a homogeneous, narrowly defined group. You are relatively alone (approximately 1% of the population meets diagnostic criteria for this condition). You have a terrible and consequential affliction. Because of your condition, you should have a protective concern for all those that cross your path. However, a key facet of your disorder is that you are incapable of developing that concern.
The name of the checklist is the Hare Psychopathy Checklist — Revised (PCL-R). The name of the disorder is psychopathy (the term sociopath is often used interchangeably with the term psychopath, but the latter is the correct, scientific term).
ln the next section l am going to try and summarize what we have learned about psychopathy. But, first, a request: l ask you to try to absorb this information on psychopathy in as dispassionate a manner as possible.
It’s a difficult request. It’s easy to have an air of clinical detachment when the pathological signs of an illness are things like white blood cell counts and abnormalities in cell structure. On the other hand, it’s also easy to be judgmental when the diagnostic signs are traits like constant lying, callousness, and remorselessness. Possession of these traits would seem to put one on the fast track to the gates of Hell. One immediately associates such traits with bad character, even evil, rather than a “condition” or “disorder.”
Those who view psychopathy as a condition are accused of “medicalizing,” which is a pejorative term describing a process of seeing bad behavior as an illness rather than a moral failing, thereby exculpating the perpetrators of bad behavior. The aim of those who “medicalize” might be to evoke more humanitarian responses to deviant behavior. But, critics would argue, to do so vitiates our moral sensibilities.
Nevertheless, this is precisely the mindset l am asking you to entertain. The research, l believe, allows me to make this difficult request. The knowledge we have obtained indicates that the psychopath is a certain kind of animal, with well-defined traits and behaviors, with predictable risk to others. And there appears to be nothing he or we can do about it.
What kind of animal exactly?
5
Our ability to answer that question — in some detail as it turns out — is largely due to the development of a rating scale, the Hare Psychopathy Checklist -Revised (PCL-R), designed to measure the degree of psychopathy in an individual. The Checklist was designed by Robert Hare, a Canadian psychologist, and his colleagues, working with a prison population in British Columbia.
They developed the checklist by listing over 100 behavioral, emotional, interpersonal and lifestyle traits that had been observed in criminal populations. They relied heavily on the work of Hervey Cleckley, considered the pioneer in the study of the “criminal mind” and author of Mask of Sanity in the 1930’s. In that book he detailed the psychopath’s often “brilliant and charming” manner, which masked a predatory nature and a lack of conscience. Through statistical analysis and studies to establish reliability and validity, Hare was able to winnow the Checklist to 22 items, which he published in 1980, and then revised to 20 items in 1991.
Although much had been written about the psychopathic personality before, Hare and his colleagues established the first systematic effort to assess and study psychopathy. The PCL-R became the gold standard, the common and objective measurement tool used to generate the research that is the foundation of our current knowledge. As a result, psychopathy has benefited from more attention and research than any other personality disorder. In addition to its solid psychometric qualities, the PCL-R emphasizes longstanding and stable behavioral and personality traits. The rating system for PCL-R requires culling life history data that can identify chronic, persistent and entrenched traits (as opposed to flamboyant criminal behavior) that we now understand are at the heart of the condition.
The PCL-R should only be administered by a qualified and trained professional. Administration is a two part process of analyzing life history data and conducting a semi-structured interview, after which the rater provides a score of 0, 1, or 2 for each of the 20 items (0= trait definitely not present; 1= information not available or there is some data to support the trait, but it is not overwhelming; and 2= trait definitely present). Hare wrote a book-length manual with extensive definitions and behavioral examples for each of the twenty traits in order to facilitate consistency and reliability of ratings.
A “perfect” score (very rare) for psychopathic tendencies would be 40. Hare set 30 to be the cutoff score for one to be deemed a clinical psychopath. Thirty was typically the cutoff score for one to be a subject in a research study on the condition, although some researchers have used a cutoff score of 25.
Here are the 20 items that the examiner is asked to provide a rating of 0, 1, or 2:
1. Glibness/superficial charm
2. Egocentricity/grandiose sense of self-worth
3. Proneness to boredom/low frustration tolerance
4. Pathological lying and deception/gaslighting
5. Conning/lack of sincerity
6. Lack of remorse or guilt
7. Shallow affect
8. Callous/lack of empathy
9. Parasitic lifestyle
10. Poor behavioral controls
11. Promiscuous sexual behavior
12. Early behavioral problems
13. Lack of realistic long-term goals
14. Impulsivity
15. Irresponsibility
16. Failure to accept responsibility for own actions
17. Many short-term marital relationships
18. Juvenile delinquency
19. Revocation of conditional release
20. Criminal versatility
Perhaps now you can see why l made the plea for clinical dispassion. The above doesn’t sound like a textbook listing of diagnostic markers, so much as a big gulp version of the seven deadly sins. Condemnation, not dispassion, feels like the appropriate response. Nevertheless, these are the traits that come out of the statistical wash to capture the condition of psychopathy. These are the traits that have established this taxonomically similar group that has produced so much research and understanding.
To which we now turn. But to be very clear: going forward, when I describe psychopathy, I will do so in a precise manner: a psychopath is one who scores at least 25 or more on the above list of traits.
6
Don’t worry, l am not going to summarize 3300 research studies. Not even close. But I’d like to start by noting some of the findings on the prevalence of psychopathy, as measured by the PCL-R. Prevalence is the proportion of a particular population found to be affected by a given condition. When the PCL-R is administered to the general population, the average score is 5. Some might find that high a score to be a troubling finding. Well, it’s certainly an acknowledgement that we are all not perfect angels. And that most of us struggle to some degree with the darker side of our nature.
When the PCL-R is administered to a prison population, the average score is 22 for males and 19 for females. That’s a big jump, and not a surprising one, given the population. Note that 22 is the average score, so in any given prison there are plenty who score 30 or above. But also note that it is still significantly shy of the criterion score of 30 for psychopathy. l hope this gives you the sense that a rating of 30 is impressive, albeit not in a good way.
Take a look at that list of traits again and let that number 30 sink in as l ask you to participate in a thought experiment. Imagine that you have an adult son or daughter. One day they call and excitedly tell you that they have been dating someone who they hope will become their spouse in the near future. Then imagine you somehow are able to secure the PCL-R rating for this prospective spouse.
l am guessing you may have the following reactions: a rating on 1 or 2 of the items gets your attention and gives you pause (after all, it is your child we are talking about); a rating of 5 or 6 may send your internal organs down a few floors; a rating of 8 or 9 gets the heart fibrillating; a rating of 12 or more sends you to the dark web to learn how to put a contract out on the prospective spouse.
So yeah, thirty is an impressive number. The prevalence in the general population of psychopaths (i.e., those who receive 30 or above on the PCL-R) is 1%. As you learn how extreme and dangerous this condition is, that 1% figure is frightening. But it’s a solid finding. We don’t appreciate how many psychopaths, these dangerous predators, are among us because some of the key traits (superficial charm, an ability to con others, lying) are designed to keep the condition hidden from others. (You may notice that I use the pronoun “he” when referring to a psychopath. Psychopathy is a condition found mostly, but not exclusively in males. The breakdown ration of males to females is around 75: 25).
Psychopathy vs. Antisocial Personality Disorder
Before proceeding to some of the key findings on the nature of psychopathy, it is necessary to provide this sidebar to explain the difference between psychopathy and Antisocial Personality Disorder. These two conditions are frequently lumped together by lay people and, not infrequently, also mental health professionals. And while there is overlap between the two conditions, they need to be differentiated, particularly for the purpose of this essay. Antisocial Personality Disorder (APD) is a formal diagnosis in the current Diagnostic and Statistical Manual (DSM-V). It is found in the Cluster B section of personality disorders. The Cluster B section contains those disorders that are characterized by dramatic, overly emotional or unpredictable thinking or behavior.
The diagnostic criteria for APD are:
- There is a pervasive pattern of disregard for and violation of the rights of others occurring since age 15 years, as indicated by three (or more) of the following:
- failure to conform to social norms with respect to lawful behaviors as indicated by repeatedly performing acts that are grounds for arrest
- deceitfulness, as indicated by repeated lying, use of aliases, or conning others for personal profit or pleasure
- impulsivity or failure to plan ahead
- irritability and aggressiveness, as indicated by repeated physical fights or assaults
- reckless disregard for safety of self or others
- consistent irresponsibility, as indicated by repeated failure to sustain consistent work behavior or honor financial obligations
- lack of remorse, as indicated by being indifferent to or rationalizing having hurt, mistreated, or stolen from another
- The individual is at least age 18 years.
- There is evidence of Conduct Disorder with onset before age 15 years.
- The occurrence of antisocial behavior is not exclusively during the course of Schizophrenia or a Manic Episode.
As you can see, there are fewer criteria for APD than psychopathy. There is also a greater emphasis on criminal and antisocial behavior. Antisocial behavior is certainly included in the diagnosis of psychopathy, but there is additional emphasis on psychological, emotional and interpersonal traits. As compared to psychopathy, APD is a broader diagnostic category. Prevalence studies indicate that 4% of the population meet diagnostic criteria for APD, approximately four times the amount for psychopathy. Clearly, not all individuals with Antisocial Personality Disorder also have psychopathy. But do all individuals with psychopathy also meet criteria for APD? The answer is: almost all. To meet all the criteria to receive a diagnosis of psychopathy pretty much guarantees a diagnosis of APD.
In the hit TV show, Breaking Bad, Walter White, the antihero protagonist — after he receives a diagnosis of stage 3 lung cancer and wants to find a way to obtain financial security for his family — transforms (“breaks bad”) from a meek high school chemistry teacher to a drug kingpin in Albuquerque, New Mexico. A big part of his success in the drug market is due to his skill as a chemist. He concocts a particularly pure form of crystallized methamphetamine that blows away the competition. His crystal meth has a blue tinge and earns the moniker “the blue stuff” on the streets of Albuquerque. Psychopathy is the “blue stuff” of Antisocial Personality Disorder.
7
What does the research tell us about this “blue stuff?”
One line of research focuses on the nature versus nurture question: “are psychopaths born to have their affliction or are they made that way by difficult circumstances in their life situations?”
The field of behavioral genetics has enabled us to understand the degree to which personality traits are inherited. The main research tool involves studying the difference between identical twins (who share 100% of the same genes) and fraternal twins (who share 50% of the same genes) on a particular trait or personality type. Since each type of twins share a similar environment, a significant difference between identical twins and fraternal twins demonstrates a genetic influence. Researchers have developed a mathematical formula — called the heritability index — to measure how much the trait is due to genetic factors. For example, we have learned that the heritability for traits such as introversion/extroversion, agreeableness and authoritarianism is between 35% and 50%.
A number of large-scale studies have zeroed in on the heritability of psychopathy. One study that followed 3,687 seven-year-old twin pairs found that “the core symptoms of psychopathy are genetically determined.” Another longitudinal study of 3,226 pairs of male twins found eight psychopathic traits to be “significantly heritable.” Another kind of study, called the Texas Adoption Project, compared the condition of psychopathy in the adopted children with both their birth parents and their adoptive parents. There was much greater similarity to their birth parents (who they had never met) than to their adoptive parents (who raised them).
There has been less success in identifying environmental factors that might contribute to psychopathy. An impoverished background is related to the risk of criminal behavior, but not to the core traits of psychopathy. A number of different types of childhood maltreatment have been investigated but, so far, no direct link to psychopathy has been found
Overall, the heritability of psychopathy appears to be over 50%. Psychopathy appears to be, to a significant degree, a condition “of the blood.” That something contributing significantly to psychopathy is inherited has been proven. But what is that something?
8
A different brain is the short answer. There is accumulating evidence that the brains of psychopaths are different than the rest of us. The development of functional magnetic resonance imaging (fMRI) has allowed us to zero in on what parts of the brain are active in relation to certain stimuli and tasks. This brain imaging technology has enabled us to pinpoint some of the distinctive features in the brains of psychopaths. The findings are striking and revelatory.
In a seminal study in 1991, Robert Hare presented a series of neutral words (e.g., table, house, tree, lap) and then a series of emotional words (e.g., love, pain, mother, hate) to a group of prisoners who scored above 30 on the PCL-R. He compared their brain activity to a group of non-psychopaths presented with the same words. The non-psychopaths reacted more intensely and rapidly to the emotional words. The psychopaths reacted to the emotionally charged words the same as to the neutral words.
More critically, the imaging showed that psychopaths processed these emotional words in the upper part of the brain (temporal lobe area) that is responsible for understanding language and problem-solving. Whereas non-psychopaths processed the emotional words in the midbrain (paralimbic area) that is responsible for emotional regulation.
These findings were reinforced in later studies by Hare and his colleague, Dr. Kent Kiehl, who is considered the leading expert on brain imaging and psychopathy. In one study, subjects with HCL-R scores over 30 were asked to rate morally offensive statements compared to neutral statements (e.g., having sex with a mother vs. listening to music). In another study, psychopaths were shown gruesome or morally offensive images (e.g., a man’s face beaten to a bloody pulp, a picture or Osama Bin Laden). Once again, the psychopaths reacted less intensely and in the part of the brain designed for language and problem-solving. They simply do not experience the appropriate emotional reactions to moral wrongs.
When almost all of us see a gut-wrenching or morally offensive situation, we automatically and rapidly react to it in the emotional part of the brain. But for the psychopath, that part of the brain seems to have gone cold. They react to such situations in a more neutral and analytic manner, tapping into the part of the brain that, for example, is trying to write a research paper. Hare notes, “it was as if they could only understand emotions linguistically. They know the words, but not the music, as it were.” They seemed incapable of empathy.
Hare, in his book Snakes in Suites — When Psychopaths Go to Work, shares an anecdote of when he was asked to consult with Nicole Kidman for the movie Malice, in which her character was supposed to display psychopathic tendencies. Hare, as a way of coaching her about the emotional life of a psychopath, gave her the following scene:
You’re walking down the street and you come across an accident at the corner.
A young child has been struck by a car and is lying in a pool of blood. You walk
up to the accident site, look briefly at the child, and then focus on the grief -
stricken mother. After a few minutes of careful scrutiny, you walk back to your
apartment, go to the bathroom, stand in front of the mirror, and practice mimicking
the facial expressions and body language of the mother. (p 54)
Another dysfunction in the emotional circuitry of psychopaths revolves around the amygdala, which is also located in the mid-brain limbic area. The amygdala is instrumental in recognizing threats and danger. It activates the (usually adaptive) fight-flight-or-freeze response when we are faced with danger, especially the danger of physical harm. But it also gets triggered when we are afraid of being punished, what many would consider a moral fear (i.e., the fear of violating acceptable rules and boundaries). The amygdala in psychopaths is much less active, which has the effect of dampening fear responses in situations where fear is adaptive or might contribute to social cohesion.
How might a muted amygdala express itself? How about a teenage babysitter — with all the good judgement typical of an adolescent — takes his five-year-old charge on an urban adventure. They venture into a sewer system under construction in Manhattan. Shortly after entering, the teenager becomes quite anxious and has second thoughts, “it was pitch black and you couldn’t see the entrance.” But the five-year-old pressed on into the gathering darkness. “The thing that amazed me,” that teenager, now turned 83 said, “was that Donny wasn’t scared. He just kept walking.”
The above anecdote, taken from the biography Trump Revealed (2016) by Michael Kranish and Marc Fisher, requires another sidebar. No anecdote, or even series of anecdotes, no matter how colorful or spot on, should be given significant diagnostic weight. I hope I have conveyed the idea that asserting a diagnosis needs to meet a high bar. To make any psychiatric diagnosis, and certainly the diagnosis of psychopathy that is the focus of this essay, you need multiple, preferably hundreds, of data points that support the diagnostic trait in question.
Yes, the above anecdote is a good example of how an under-functioning amygdala might express itself. But it does not prove Donald (“Donny”) Trump has an under-active amygdala or is a psychopath. It is just one suggestive data point where many more are needed to confirm the tendency. I also want to emphasize that the above anecdote (and all others to follow) would not have been used if it was solely based on Donald Trump’s self-report. Some of Donald Trump’s telling of his early years seems apocryphal and designed to create an impression of a tough guy and maverick. For example, he frequently recounts that when he was in the second grade, he punched his music teacher, giving him a “black eye” because “I didn’t think he knew anything about music.” However, the music teacher, who died in 2015, never confirmed the story and none of his friends from that school recall such an incident. Data points that have some external validation are preferable to one’s based on the subject’s self-report.
On September 13, 1848 Phineas Gage, the foreman of a construction crew laying down railroad tracks in Vermont, suffered a grievous accident. He was using a tamping rod to pack down explosive powder into a hole, and the power detonated unexpectedly, propelling a 43-inch-long and 1.25-inch diameter rod up thru his left cheek, obliterating a section of his brain, before exiting his skull and landing eighty feet away. Amazingly, Gage walked back to his lodgings and summoned a doctor. When the physician rode up, Gage greeted him, “Doctor, here is business enough for you.”
Thus, Phineas Gage became one of the more famous cases in cognitive neuroscience history. The damage from the accident was limited to a portion of the prefrontal cortex. The changes Gage displayed after the accident enabled us to learn about the specific brain functions of that area of the brain. Before the accident, Gage had been described as considerate, mild-mannered and hard-working. Afterwards, he was described as coarse, abusive, dishonest, and incapable of restraint when it conflicted with his desires. He was no longer able to control his impulses. The prefrontal cortex has been described as the personality center of the brain. It helps us control our impulses and serves as a braking system, so we don’t act without considering the consequences. It enables us to defer immediate gratification for long term rewards. Psychopaths have been found to have less grey matter in this area of their brains. Their brains also show less connectivity between the prefrontal cortex and the amygdala, thus compromising their ability to integrate rapid-fire impulses with reason.
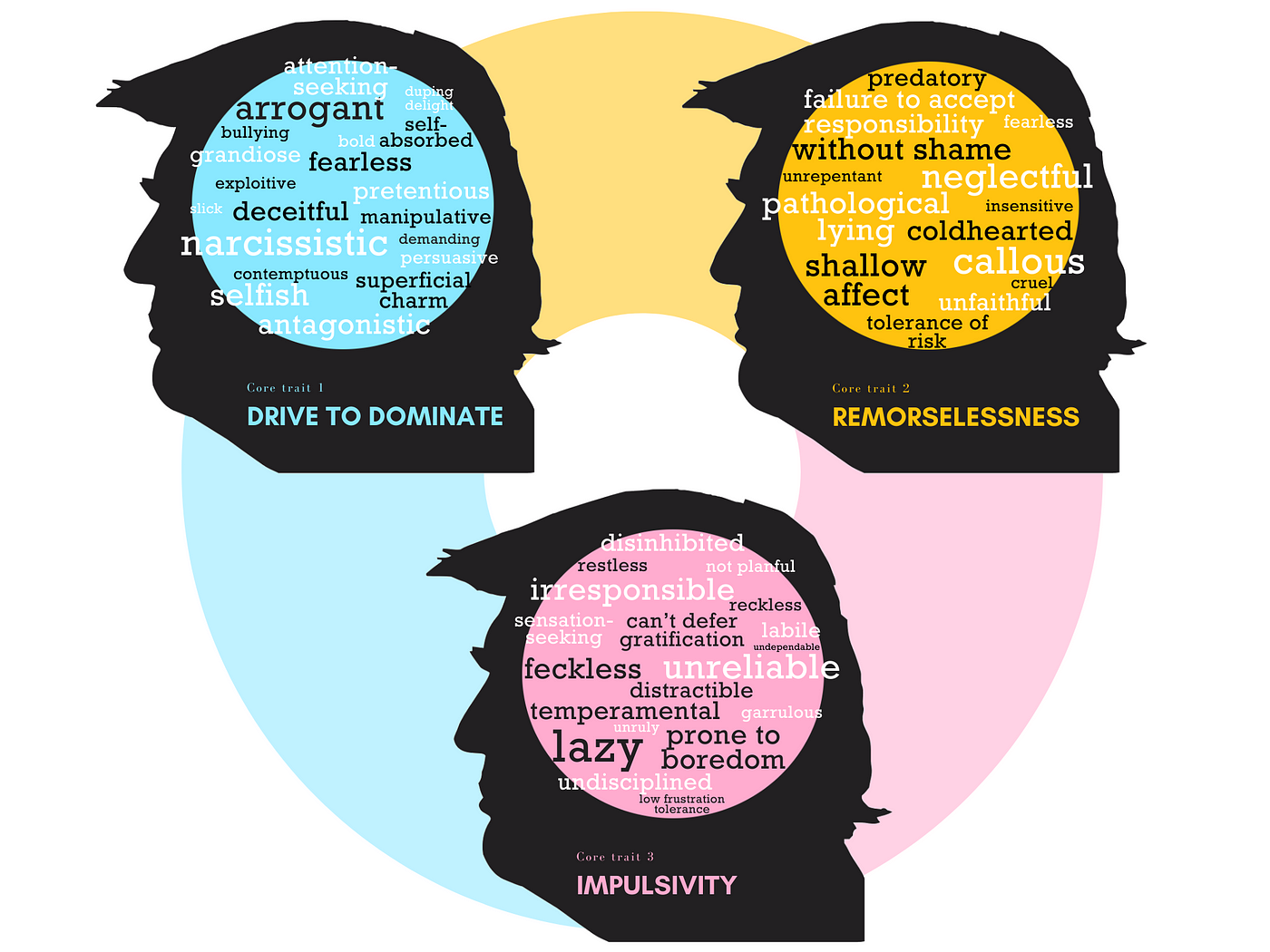
So, we now know some of the neurodevelopmental deficits inherited by psychopaths. The abnormalities in the limbic area, amygdala, and prefrontal cortex are in areas of the brain that are implicated in the core emotional and behavioral traits displayed by psychopaths. While the Psychopathy Checklist contains twenty such traits to help make the diagnosis of psychopathy, the abnormalities in these three areas of the brain help explain three fundamental traits that appear to be foundational to the condition:
the lack of conscience, due to the inhibition of moral fear and absence of states of guilt and shame; the inability to process emotions that foster empathy and human connection; and the inability to control impulses
While biology is not total destiny, the burden of these brain deficiencies is hard to overcome. Psychopathy, remember, has a heritability factor of over 50%. And if you are on the wrong side of that fateful genetic coin toss, well then… from the mouth of one well-depicted psychopath … You would be inheriting a condition that is antithetical to much of what we associate with being human. A condition that consigns one to a bleak and blinkered life or, as one Trump biographer put it, “an existence unmolested by the rumblings of a soul.” This is where you think about taking a bullet to protect your child from acquiring such a condition.
9
You have seen the list of traits that define the condition, but what is it like to be a psychopath? To acquire that understanding we can’t turn to the psychopath himself. There are few first-person accounts of psychopathy. And other than descriptions of the cold-bloodedness they bring to their crimes and transgressions, they provide little insight into the experience of being a psychopath. And, no wonder, psychopathy is mostly about the absence of human qualities. It would be like asking someone to describe a color to which they have been born blind.
Works of fiction and journalism are pretty much restricted to the stories of serial killers, and therefore can be misleading about the wider population of psychopaths (although Norman Mailer’s Executioners’s Song has much to recommend it).
The best source for understanding the world of the psychopath comes from those clinicians and researchers that have devoted their attention to it. One of the best is Martha Stout, author of the bestselling The Sociopath Next Door (2005). She starts her book with a thought exercise that, er, might remind you of someone:
Imagine — if you can — not having a conscience, none at all, no feelings of guilt or remorse no matter what you do, no limiting sense of concern for the well-being of strangers, friends, or even family members. Imagine no struggles with shame, not a single one in your whole life, no matter what kind of selfish, harmful, or immoral action you have taken…Now add to this strange fantasy the ability to conceal from other people that your psychological makeup is radically different from theirs. Since everyone simply assumes that conscience is universal among human beings, hiding the fact that you are conscience-free is nearly effortless…You can do anything at all, and still your strange advantage over the majority of people, who are kept in line by their conscience, will most likely remain undiscovered…Maybe you are someone who craves money and power, and though you have no vestige of conscience, you do have a magnificent IQ. You have the driving nature and intellectual capacity to pursue tremendous wealth and influence, and you are in no way moved by the nagging voice of conscience…You choose business, politics, law, banking, or any of a broad array of other power professions, and you pursue your career with a cold passion that tolerates none of the usual moral or legal encumbrances. When it is expedient you doctor the accounting and shred the evidence, you stab your employees (or your constituency) in the back, tell lethal premeditated lies to people who trust you, attempt to ruin colleagues who are powerful or eloquent, and simply steamroll over groups who are dependent and voiceless… You have a special talent for whipping up other people’s hatred and sense of deprivation… And all this you do with the exquisite freedom that results from having no conscience whatsoever…You become unimaginably, unassailably, and maybe even globally successful. Why not? With your big brain, and no conscience to rein in your schemes, you can do anything at all. (p. 1)
It should be noted that Stout wrote this before Trump walked onto the political landscape. It is unlikely she had him in mind. She was describing a common trajectory of a psychopath, not a particular individual. Experts on psychopathy place this lack of conscience, this remorselessness at the center of the disorder.
Items from the Psychopathy Checklist (PCL-R) that seem to flow directly from the absence of conscience include pathological lying, lack of remorse, history of juvenilely delinquency, conning, and having more than one type of criminal offense. To have a conscience is such a deep, innate part of being human, it is difficult to imagine not possessing one. It’s hard to imagine having no fear about being found out for moral transgressions, no compunction about lying, and no gut-level reservations about acts that might harm others. Not having a conscience is like having a car without brakes.
Conscience is the glue that keeps the social fabric from unraveling. It undergirds the social contract that promotes decency, safety, and trust. Yet there is that small percentage that live outside that social contract, that 1% who, in the apt phrase of Hervey Cleckley, “carry disaster lightly in both hands.” Is it not desirable to identify those without a conscience, particularly if they are in a position of power over others?
10
Well, one could argue, the inability of the brain and nervous system to generate the inhibitory emotions of guilt, shame and fear — that are foundational to developing a conscience — doesn’t have to result in predatory or harmful behavior. Just because one lacks the capacity to feel bad about doing bad, doesn’t necessarily mean one can’t feel good about doing good. Just because one is not constrained by feelings of guilt or shame, doesn’t mean one can’t be motivated by feelings of love or virtue.
However, this is where we careen into the second ditch in the psychopath’s interior landscape: the inability to empathize or care deeply. This was the central trait Cleckley noted in Mask of Sanity, “beauty and ugliness (except in a very superficial sense), goodness, evil, love, horror, and humor have no actual meaning, no power to move him.” We have already noted that when images of suffering are presented to the psychopath, there is no activity in the emotional centers of the brain. It is an ice station as far as empathy and deep caring are concerned.
Martha Stout makes a link between the difficulty to form a deep bond with others and the absence of a conscience. She defines conscience as the “intervening sense of obligation based on our attachment to others.” But if someone simply cannot experience the deeper feelings of love, tenderness, or compassion, then they have no motivation to protect, sacrifice, or feel responsible. If others just don’t matter much, there is no motivation to build a conscience. Instead of expressions of empathy, there are acts of callousness.
This missing gear to connect deeply is reflected in the marriages of psychopaths. Stout notes, “once the surface charm is scraped off, their marriages are loveless, one-sided and almost always short-term. If a marriage partner has any value to the sociopath, it is because the partner is viewed as a possession, one that the sociopath may feel angry to lose, but never evoke sadness or accountability.”
However, it would be misleading to suggest that the psychopath is disengaged entirely from relationships. Experts in marital therapy and interpersonal communications note that in any serious relationship there is a complex dance that revolves around two questions: (1) “how close do l want to get to this person?” and (2) “who is on top?” In serious relationships, there is this ongoing dance of intimacy and power. The psychopath does not have the neurological infrastructure to even get on the dance floor of intimacy. But he is kinetic with dance moves of asserting power.
Since dominance and “winning” is the only dance card available to him, the psychopath often becomes adept at it. His focus is one-dimensional and aggressive (“grab ’em by the pussy”). He concentrates on immediate gains and gratifications driven by his egocentric needs. Relationships are instrumental. People are means, not ends, in themselves.
And the psychopath has plenty of emotional fuel. Admittedly, not the animating force that flows from love, compassion and empathy; but emotions associated with the drive to dominate such as anger, glee, resentment. envy, consternation, jealousy, and contempt. These emotions are shallow and often fleeting, but can be intense in the moment, and typically drive the psychopath’s behavior.
The psychopath is out to dominate his relationships. That is his exclusive goal. He may recognize (cognitive empathy) the rewards for acting as if he cares for someone. And this self-interest may serve as a check on his behavior for a while. He may even enter professions where the opportunities for prosocial behavior abound — medicine, law, politics, business, and even religion. But exploitation and harm eventually win out.
Over time, this wiring of the psychopath, which doesn’t allow him to care, but only operate in the gear of “winning” in a relationship (whether with a spouse, friend, colleague, or country), means that he will always be drawn to actions that benefit him and disadvantage the other. This may start out as mere selfishness and lack of reciprocity, but inevitably moves to dereliction and cruelty.
Specific items from the Hare Psychopathy Checklist that are linked to this core inability to empathize and care include: promiscuous sexual relationships, callousness, parasitic lifestyle, frequent marital relationships, shallow affect, and the tendency to be cunning and manipulative.
To not be able to care deeply is an affliction. It is sad (seriously). But to be in a relationship with such a person is risky. It is not only driving a car without brakes (lack of conscience), but also a car that can only operate in one gear (domination) that will eventually strip the transmission (relationship) to shreds.
But wait…it gets worse.
11
David Shapiro, author of the classic text, Neurotic Styles (1965), made groundbreaking observations of the psychopathic condition, which he saw as a variant of a more general impulsive mode of limited functioning. He was able to bring to life the narrow bandwidth of the psychopath’s consciousness and pinpoint the deficiencies that constitute this sad, but also dangerous condition. His observations were prescient: they anticipated the findings of brain research conducted later.
Shapiro describes the psychopath as one who is enslaved to his impulses and whims. As he goes through the day, the psychopath is not able to engage the world beyond the immediately present and personally relevant (“what’s in it for me?”). For the psychopath, an impulse is not something fleeting, to be evaluated in the context of deeper interests, long-term goals or moral concerns. For most of us, an impulse — triggered easily and often in the more ancient, lower, emotional parts of our brain — evokes the beginning of a process, where the impulse is mediated by the higher functions of judgement, self-control, and conscience, located primarily in the cerebral cortex.
But not for the psychopath. For him, the impulse — triggered by the immediate frustrations and opportunities of the moment — is acted out quickly. The behavior of the psychopath is therefore labile and erratic. It can turn this way or that based on his rapid-fire “what’s in it for me?” appraisal of the immediate situation. The behavior is egocentric and, often exploitive. This was Phineas George after his accident. This can be college sophomores at a party who engage in binge-drinking and are then at significant risk for sexual assault because the excessive alcohol shuts down that part of the brain that curbs impulses.
The feelings that accompany this impulsive style are shallow and primitive, typically restricted to the arena of pain vs. pleasure, and frustration vs. gratification of the immediate situation. Since there is a diminished capacity to process emotions in the higher levels of the brain, there is no refinement of feelings that occurs when impulses are weighed against long-term interests or the strictures of conscience.
For the psychopath, life is ruled by impulse. Their attention is easily captured and rarely goes beyond the egocentric interests of the concrete present. Impulse is not occasional, but regular. Impulse is not the beginning of a process of weighing, deliberating and mindful choosing, but the short-circuiting of it.
Shapiro emphasizes that this “life ruled by impulse” does not represent a disruption of executive functioning, but rather a deficiency of executive functioning. When an impulse is triggered, the deficiencies in these higher-level mental functions means there is no counterweight to it.
Imagine a married man with this condition who meets an attractive woman at an out of town conference and, in sizing things up, believes he can hook up with her. His ability to measure what might be tempting in the moment against what it might mean in two months is…just not there. Nor is the predisposition to weigh the moral consequence of such a sexual encounter. The calls most of us make every day between “l want” vs. “l should” just don’t take place with a psychopath. He has only one play available to him: the short game of winning the moment.
Thus, the behavior of the psychopath should not be viewed so much as immoral, as amoral. He is not violating his moral scruples. He is simply acting sensibly with regard to the opportunities of the moment. That such behavior is predatory is a problem for people in his orbit, not for him. Elizabeth Stout emphasized the psychopath’s inability to develop a loving bond with another. David Shapiro would argue there is a more fundamental inability to develop any deep allegiances: to a significant other yes, but also to friends, the community, even ideas and values. The cognitive and affective infrastructure to develop stable and deeper interests and bonds is…just not there.
This inability to develop aims and values beyond the immediate tangible gain should not be confused with a lack of intelligence. Indeed, as Shapiro observes, it can convey certain advantages:
It is well to remember, however, that the impulsive style may, in certain areas of living, be quite adaptive. These areas seem, in general, to be ones where readiness for quick action or expression and/or a facility and competence of a sort that be developed in pursuit of immediate and egocentric interests can be useful. It is well known, for example, that many impulsive people possess considerable social facility and are often socially very charming and engaging. They may also be quite playful, in contrast, for instance, to the heavy, over deliberate, and somewhat dull quality of some obsessive-compulsive people, and, given a good intellectual endowment, they may be witty and entertaining. There is no doubt also, that many actual as well as fictional “men of action,” have excellent practical competency and a capacity for quick and unhesitating action… have a keen, practical intelligence that is suited to the competent execution of their short-range, immediate aims. (p. 147)
It is not surprising that some psychopaths attain significant wealth and power, given their cunning and singular drive to dominate. Pathological lying, one of the twenty items on the Hare Psychopathy Checklist, can be understood as an expression of this impulsive style. Pathological lying, as operationalized in the Checklist, does not refer to the enormity of a lie, but to its frequency. A big lie (e.g., promoting a fraudulent university) usually requires some planning and deliberation. The big lie, of course, represents problematic behavior and is related to the psychopathic condition. However, it is accounted for in the Checklist in the item labelled “conning.”
Pathological lying refers to lying frequently. The quality of such lying is casual, glib, “off the top of the head” (see his riffs at his rallies and debate performances for good examples of this style). The pathological liar often contradicts himself within minutes (but shows scant concern for the contradiction). The lying can occur over what seem like the most trivial of matters. The impulsive mode helps explain this trait. The psychopath is stuck in the gear of winning the moment, “getting by,” “operating” (in business vernacular “always working on the closing”). The lying is often an embellishment, meant to impress or gain an advantage, even if only slightly. And he is at the mercy of saying quickly whatever meets his egocentric needs of the moment (there are many examples of this behavior from his press briefings in the early days of the coronavirus crisis, where he would say something that ‘won the moment’ but needed to be immediately corrected by experts). He has no buffer of aims or values to deflect the drive for the immediate, tangible gain. Consequences to others are not in his purview.
The psychopath is not interested in what is being said, but how it works for him. Logic, objectivity or the simple desire to be truthful are not part of his mindset. Truth is transactional. The psychopath speaks power to truth. Items from the Hare Psychopathy Checklist that emanate from this impulsive mode of functioning include glibness/superficial charm, short-tempered/poor behavioral controls, pathological lying, lack of realistic long-term planning, promiscuous sexual relationships, and superficial emotional responsiveness.
To live a life ruled by impulse is like driving a car without a GPS. To be caught in traffic with such a car is hazardous, because the car also has no turn signals or brake lights and is prone to jerking this way or that without any concern for its fellow drivers. And the driver of the car? Well, he has all the self-control of a Don Draper chugging his way thru a bottle of gin.
12
These three cardinal traits — absence of conscience, inability to empathize or bond deeply with others, and impulsiveness — are at the heart of the disorder and mark psychopaths, in Elizabeth Stout’s words, as “a group unto themselves.” They lead a life driven by egocentric impulses, which are unmodulated by conscience or concern for others. They lack the humanizing and self-control functions which most of us take for granted.
To re-visit the car analogy, this psychopathic model, while it may look sleek, is hazardous. Remember, it has only one gear (to dominate), which is destined to shred the engine and no brakes (conscience). If you could somehow get this vehicle to a repair shop before it was totaled in an accident, and raise it up on a hydraulic lift, you would discover that there is no repair called for, no damage to be fixed. Rather, you would see that there simply is no system of brakes, no multiple gears, no GPS. These basic systems necessary to drive a car safely are…just not there.
Of course, with a car, you could order the missing parts and replace these missing systems. And it’s true with the human body we are now capable of replacing major organs such as the heart, kidney or lungs. But we don’t yet have the medical technology to replace missing parts of the brain. l mean Dr. Frankenstein tried, but we saw how that turned out.
To be in the path of a psychopath is to put oneself in harm’s way. The risk to others is inherent in many of his destructive personality traits — deception, lying, breathtaking callousness, engagement in more than one type of criminal activity. For a psychopath who is in a position of significant power and authority, other manifestations of his condition bode ill for those under his sway. These would include the inability to act predictably, the inability to react calmly and without aggression, the inability to examine his own behavior and accept responsibility, the inability to respect boundaries and limits, and the inability to place the interests of others or the common good above his own.
All of these tendencies have the gravitational pull of a black hole. Over time, the social network over which the psychopath has influence, slides toward disruption and deterioration. This storm of ruinous traits is not going to dissipate. No repair is possible. The best we can do is recognize its presence and try to protect ourselves.
Before we turn to the 45th President of the United States and the thesis of this essay, I’d like to underscore what we now know about psychopathy, the substance beneath the chilling Hollywood image of a character like the Joker. What we can say with authority:
- Psychopathy — defined by a score of 30 or more on the Psychopathy Checklist — is a coherent syndrome, with well-defined and relatively stable traits and behavioral inclinations;
- The condition can be reliably diagnosed by a trained professional;
- 1% of the population displays this condition;
- The condition is stable. It surfaces in childhood and does not abate significantly over time;
- We have identified a number of neurological deficits that help explain some of the core features of the condition;
- Very few psychopaths seek help for their condition. But if they were to, there is no effective treatment to offer them;
- Psychopathy is a unique form of psychopathology in that it does not involve suffering by the psychopath himself. The main consequence of the condition involves the danger it poses to others.
If someone merits this diagnosis based on their score on the Hare Psychopathy Checklist, there is “a lot we can say about him” — about his deeply ingrained traits and behavioral tendencies, the unalterable course of his disorder, that he is refractory to any kind of treatment, and, most critically, the risk he poses to those in his dominion.
So, does the President meet the cutoff criteria of The Psychopathy Checklist? Is he a predator, without conscience, incapable of controlling his impulses?
13
In order to answer this question with credibility, it is first necessary to address two threshold questions:
- Can we make such a diagnosis? That is, are we in a position to even attempt a diagnostic inquiry, given that we are not able to interview the individual (Trump) in question?
- Should we attempt a diagnostic assessment? Is it ethical to diagnose a political figure “from a distance?”
These two questions are compelled by an ethical constraint on mental health professionals called the Goldwater Rule. The Goldwater Rule is found in section 7.3 of the American Psychiatric Association’s (APA) code of ethics and asserts that it is unethical to offer a professional opinion on a public figure that has not been personally examined and where consent has not been obtained.
These ethical guidelines are called the Goldwater Rule because, during the 1964 Presidential campaign, FACT magazine (now defunct) invited psychiatrists to participate in a survey of the psychological makeup of candidate Senator Barry Goldwater. Psychiatrists that responded branded Goldwater with various diagnoses and descriptors, such as “paranoid,” “schizophrenic,” “psychotic,” and “narcissistic.” Most responders claimed Goldwater was “dangerous” and unfit to be President.
Goldwater later successfully sued the magazine for libel. The verdict in that case and the episode as a whole was damaging to the reputation of mental health professionals. During the 2016 Presidential campaign and continuing with the ascension of Trump to the Presidency, there has been much debate of the Goldwater Rule among mental health professionals. Many have argued that the “duty to warn” the general public about the danger of the Trump presidency is a competing ethical concern that compels them to override the Goldwater Rule.
But the rule remains in effect. It was reconfirmed in 2016 by then-President of the American Psychiatric Association, Maria Oquendo, as she stated “simply put, breaking the Goldwater Rule is irresponsible, potentially stigmatizing, and definitely unethical,” and then-President of the American Psychological Association, Susan McDaniel echoed, “the American Psychological Association wholeheartedly agrees with the American Psychiatric Association that neither psychiatrists nor psychologists should offer diagnoses of candidates or any other public figure they have never examined.” Thus, the answer from the two major mental health organizations to the questions “can you?” and “should you?” [diagnose at a distance] is an unequivocal “no,” and any member who does so is deemed to be behaving unethically.
Who has the upper hand in this debate over the Goldwater Rule? Fortunately, we can turn to a paper that provides a thorough, thoughtful and scientific critique of the Goldwater Rule (Lilienfeld, Miller and Lynam, 2017). In particular, Lilienfeld and colleagues (2017) address the “can you?” question as to whether you can conduct a valid psychodiagnostic inquiry without interviewing the individual in question. They make a strong case that you certainly can, and that the clinical interview should not be considered the “gold standard” of diagnostic assessment.
They note there are three sources of information that can be tapped to conduct an ideal diagnostic evaluation:
- Information from the subject himself (this is the clinical interview, which typically lasts between 1–2 hours and may include administration of questionnaires and other psychological measures)
- Informant data. Information from observers (this would include information from informants such as family, friends, colleagues, employees, golf partners, etc. If the person is a celebrity, this information may be obtained from well-researched biographies and interviews).
- Information from what are called archival sources (e.g. speeches, tweets, taped interviews, autobiographical efforts, court records, real time observations, etc.)
The assumption that the clinical interview is the most valuable and valid source of information is not supported by various lines of research. The research on cognitive bias shows that interviewers often display errors in judgement, such as overvaluing flamboyant or dramatic information in their judgement process. They are also susceptible to impression management, which refers to the interviewee’s desire to create a good impression which can lead them to distort their self-report. Studies reveal that interviewers exaggerate their ability to detect such impression management.
These concerns are amplified when you might be evaluating a psychopath who is so facile with lying and is not prone to view his problematic behavior as pathological. Indeed, in one study with psychopaths, the diagnostician’s ability to predict future behavior was actually diminished when an interview was added to the case file data.
There are a number of reasons why informant data yields higher validity than information from the clinical interview. Informant data can consist of reports of scores of individuals who may have known the subject for many years and observed him in different roles. Different sources of information provide non-overlapping data, contributing to incremental validity. Such data can provide evidence of persistency (a diagnostic trait displayed over time) and pervasiveness (diagnostic trait displayed across situations), that are instrumental in making the diagnosis. Informant data also allows the diagnostician to take advantage of statistical aggregation, which minimizes random error by cancelling out idiosyncratic viewpoints of individual informants, and converges their shared viewpoints.
Because of the many biographies and investigating reporting available on Trump, there is extensive informant data. There is also a wealth of archival data, in large part due to the televised nature of celebrity and the modern Presidency. There are thousands of hours of videotape available for behavioral observation of relevant diagnostic markers. The internet is another storehouse of information on Trump. It is hard to imagine another individual for which there is such abundant, high-quality information, which provides so many data points for a diagnostic evaluation. This is fortunate since it enables us to meet the rigorous requirements spelled out in the Psychopathy Checklist manual. The arguments and evidence summarized by Lilienfeld and colleagues (2017) dismantle the core assumption of the Goldwater Rule: namely the necessity and primacy of the clinical interview. Informant and archival data provide higher validity than information gained from the interview.
We should also note the unreliability of interviewing someone who has every incentive to minimize discussion of unreliable traits. And (if it turns out he meets diagnostic criteria for psychopathy) whose natural mode of interaction is “operating” and lying to create a good impression.
Therefore, the Goldwater Rule does not have an empirical leg to stand on. The answer to the question “Can you perform a valid diagnostic evaluation without a clinical interview?,” is an unqualified “yes.” Having established we can validly diagnose public figures “at a distance,” the question remains as to whether we should do so. Those who support the Goldwater Rule and argue we should not, raise two fundamental concerns: (1) potential harm to the reputation of the public figure, and (2) potential harm to the reputation of mental health professionals.
Calling Barry Goldwater’s mental health into question was stigmatizing and harmful to him. The Goldwater episode also stained the reputation of mental health professionals who were seen as making politically motivated, unsubstantiated claims about Goldwater’s mental health and fitness for office. The Goldwater Rule was an understandable response to armchair diagnosis that lacked a scientific foundation. Certainly, one lesson of the Goldwater affair is to approach diagnoses of public figures with caution, humility and rigor.
Those on the should side of the ‘diagnose at a distance’ argument, typically invoke the “duty to warn” principle, that places an ethical obligation on mental health professionals to warn third parties if they determine that a client under their purview is a threat to harm them. This duty to warn stemmed from a court decision in California in 1976 (the Tarasoff case). The “duty to warn” guideline, many now assert, should also be exercised when mental health professionals determine that a public figure represents a danger to society.
Lilienfeld and colleagues (2017) offer another guideline, which they call the “duty to inform.” Duty to inform has a different threshold for professionals deciding whether to make public comments on politicians. A core value in a democracy is an informed citizenry. Citizens have a right to any information that is relevant and meaningful for those in office or seeking office for positions of power that affect the general welfare. This would include, but not be limited to, considerations of dangerousness.
In the contemporary era, candidates and office holders are expected to disclose critical information about their health and competency. If a candidate for high office was diagnosed with an incurable neurological disease that affected his or her judgement, we would feel entitled to that knowledge. If a candidate was diagnosed with acute myeloid leukemia and thus not expected to survive his or her term in office, we would likewise feel entitled to know. If an individual in public office has a condition that guarantees he will inflict harm on others, we need to know. While the “duty to inform” proposal opens the door more widely to the diagnosis of public figures, it does come with a major caveat: that mental health professionals refrain from any judgements about the candidate or office-holders fitness for office. Valid diagnostic information that can contribute to such deliberations is encouraged, but conclusions regarding fitness for office are better left to the legal and political arenas. But the right to important health information about individuals running for or holding an important public office seems unimpeachable.
Alright then, we have made the argument we can diagnose Donald Trump at a distance, as well as the argument we should do so. We now turn to the question of “how.” How, exactly, are we to accomplish this task?
14
The first part of the answer to that question is obvious: we will use the Hare Psychopathy Checklist-Revised (PCL-R). Just to remind you of its bona fides, the PCL-R is the cornerstone for a deep and wide-ranging understanding of possible psychopathic individuals. Any diagnosis derived from it is based on an extensive empirical foundation, painstakingly constructed over the past 40 years by studies of the construct of psychopathy.
The competent administration of the PCL-R requires professional training and experience. Because of their training in test theory, psychometrics, and behavioral observation in research settings, I would argue that clinical psychologists might be the best candidates for this diagnostic task. It goes without saying that familiarity with the literature on personality disorders is also a must.
The PCL-R not only provides us with a reliable instrument that yields a valid diagnosis, but also spells out a rigorous process for how to go about making a possible diagnosis. This process involves the collection, integration, and interpretation of multiple sources and types of information. The process is comprehensive and detailed and strives to go well beyond just citing examples of Trump’s more outlandish behavior as definitive proof of a psychiatric disorder.
The first major task involves the collection of relevant information. We should acknowledge at the outset that this will not include any information gleaned from an interview with Trump since he would never consent to such a thing. However, we again should note there is research to support the position there is an unwarranted mystique in the importance of the clinical interview (the key component of the Goldwater Rule), especially with personality disorders.
Not to worry, because there is, um, an abundance of informant and archival information on the guy. A partial list of sources would include: (a) 13 autobiographical efforts (according to his Wikipedia page); (b) 63 biographies, many of which are richly sourced; © hundreds of interviews from print, radio, and television; (d) over 17,000 tweets since he announced his candidacy; (e) social media material from his Facebook page and YouTube productions; (f) court records; (g) details of financial dealings that made into the press; and (f) investigative reporting…well, you know this already. Trump is arguably the most chronicled celebrity/President/person in history. The wealth of information is good news for one attempting to ascertain a diagnosis. But also, overwhelming.
How does one go about integrating so much information? The process is one of prioritizing, winnowing and collating the material. Training as a diagnostician, coupled with guidelines Robert Hare laid down in his manual for the checklist, enabled us to prioritize certain batches of information over others. Some of these key priority informational “markers” include:
- Information from his childhood, adolescence and young adulthood. The condition of psychopathy expresses itself early in life. Data is needed from these earlier stages of development to make an assessment.
- Information in which the trait is expressed in overt behavior (e.g., an instance of his lying is privileged over an accusation of his lying).
- Information that reflects his typical functioning and lifelong patterns vs. descriptions of more flamboyant, occasional behavior.
- Information that is well-resourced, substantiated and has some type of external validation.
- Behavior that lends itself to coding and thus quantification (e.g., number of documented lies, lawsuits, or grandiose statements).
Even using these markers to sift through the mass of information, we are still left with thousands of instances (which we will now refer to as data points) of Trump’s behavior that are relevant to the Checklist items. The interpretation process involves taking one item at a time (in a few instances, two related items can be combined) and cull all the data points that support it. Hare proscribes a particular order to this item-by-item analysis. We then have however many data points assigned to each item. Now we are in a position to generate a score.
Remember, each item is assigned a score of 0 (trait definitely not present), 1 (information not available, or there is some data to support the trait, but it is not overwhelming), or 2 (trait definitely present). The designation of a 2 for an item deserves some elaboration. Hare emphasizes that a perfect match is not necessary to justify a rating of 2, but rather “a reasonably good match in most essential respects: the behavior is generally consistent with the flavor and intent of the item, even if only a few of the characteristics are displayed, providing that, in the rater’s opinion, they are sufficiently extreme in intensity, frequency or duration.” (Hare, 1991, p. 6). Thus, for example, even though many of Trump’s business dealings may have been above board, what we have learned about the fiasco of Trump University (as well as a number of other shady business dealings), warrants, in my judgement, a 2 for “conning” (item #5).
Here are my ratings for the 45th President of The United States:
- Glibness/superficial charm — 2
- Egocentricity/grandiose sense of self-worth — 2
- Proneness to boredom/need for stimulation — 2
- Pathological lying and deception/gaslighting — 2
- Conning/lack of sincerity — 2
- Lack of remorse or guilt — 2
- Shallow affect — 2
- Callous/lack of empathy — 2
- Parasitic lifestyle — 0
- Poor behavioral controls — 2
- Promiscuous sexual behavior — 2
- Early behavior problems — 1
- Lack of realistic long-term goals — 0
- Impulsivity — 2
- Irresponsibility — 2
- Failure to accept responsibility for own actions — 2
- Many short-term marital relationships — 2
- Juvenile delinquency — 1
- Revocation of conditional release — 0
- . 20. Criminal versatility — 2
Total = 32
Thirty-two (32) is a serious number for this instrument. Thirty-two means you are a 1%. Recall that the mean number for male prisoners is 22(!). So, yeah, 32 is substantial. In law enforcement vernacular, an individual with this score would be termed a “stone-cold psychopath.
That is the essential question. But a sidebar first, l believe, is in order. To have confidence in the assessment put forward in these pages, the reader needs to know, of course, that the examiner is competent. But also fair-minded. Not biased or politically motivated. This requires some sharing of my story.
l am a registered Democrat. Have been all my life. ln this century, I have knocked on a lot of doors for Kerrey, Obama, and Clinton. Am currently involved in efforts to counter voter suppression. Democratic blood runs in our family. My grandfather, Arthur H. Greenwood, served in the House of Representatives from 1923 thru 1939, representing districts in southern Indiana. He was the Whip in the House under Roosevelt from 1933–1935 and helped shepherd through New Deal legislation.
Currently, I oversee a therapy practice in Washington D.C. l have spent no small number of hours trying to respond to clients who are in acute distress over the behavior of the President. Feelings of disillusionment, anger, and anguish are daily occurrences for my friends and I. l have turned to reading and writing (see Into Asphyxiated Air — My Empathy Trek with Trump) as a way of trying to understand how this could have happened to our county. To little avail, I should add.
The motivation to put together this essay flows from my political sensibility. To be sure, I have a proverbial dog in this fight. I want to contribute to the effort to prevent his reelection. Sure do.
Nevertheless, that does not prevent me from making an objective diagnostic assessment that stands on firm scientific ground. To deviate from that standard would be, among other things, stupid and counterproductive. As discussed earlier, the Goldwater Rule is antiquated and does not pose a barrier to making a diagnosis at a distance. Also, there is abundant data available to make such a diagnosis of Trump. Mental health professionals have a right, some would say a duty, to inform; and, more importantly, the capacity to do so. Of course, they still need to conduct the assessment without bias.
If bias were to occur, it would express itself in the ratings l gave Trump on the items of the PCL-R. If you think the rating is inflated, l would argue “go to the tape.” Reexamine those items in the Checklist and hold them up to Trump’s chronicled behavior. Even Republicans would admit (okay, maybe with some truth serum) that the rating is in the ballpark. The rating reflects a fair-minded effort to call balls and strikes. On a few items l gave Trump a “1” there is a credible argument he could have been given a “2.” If you bent over backwards to give Trump the benefit of the doubt on each item and he received a significantly lower ranking (25 let’s say), we are still in very dangerous waters.
I certainly want to put out a request: that any licensed mental health professional with a background in the assessment of personality disorders, conduct their own evaluation of the President. The data is available. You don’t have to be a Pre-Cog. All you need to do is put in the work. It would be particularly helpful for such professionals who are registered Republicans to weigh in. Their reactions to this essay would also be appreciated.
15
To return to the question, “what does it really mean to have such a high score on the Hare Psychopathy Checklist?” Let’s start with the declaration that we are all more human than otherwise. And that we all have an inborn fallen nature. We all struggle and often fail to be our best selves. This is a given. But this score is not a measurement of someone’s struggle on the road to developing character. It is something altogether different. This high a score means the President has a condition. He is a clinical psychopath (in the moderate to severe range). It is a condition with a particular set of destructive traits that appear to have brain dysfunction underpinnings.
To receive such a score is to be set off from the great majority (99%) of the rest of us. It is similar to the man receiving a diagnosis of Acute Myeloid Leukemia, who is then distinguished from most of us by dint of his aberrant blood chemistry. Clinical psychopathy is a condition as differentiating and undeviating as a primary color. Yes, there are different shades of red, but no one should mistake red for blue or yellow. So, what does it mean to have such a high score, to be a “stone cold psychopath?” It means that person has about as much chance of controlling their impulsive, remorseless, predatory behavior as a mosquito does of not drawing blood from sweaty revelers at a state fair. A creature is going to do what a creature does.
Yes, we are all more human than otherwise, but this diagnosis carries empirically supported predictions with it. Warnings, really. The observations that our democracy is at a tipping point, and that Trump’s divisive, norm-shattering behavior are instrumental in bringing us to this denouement, are, at this point, all too familiar. His high score on the PCL-R validates those observations. It sadly reinforces the reality that the possibility of his amenability is scant and that the following outcomes — because they are inherent in this condition — are inevitable:
- Because of his greater than normal need for stimulation, coupled with his impulsivity, disruptions to the legal, financial, and administrative functions of our government will accumulate.
- In the exercise of his duties, at every choice point, power and dominance will likely prevail over the welfare of others.
- Because of his inability to process emotions related to danger, the government will be less responsive to threat situations (hello, coronavirus).
- Because he is undaunted by fear of punishment, norms of trust and decency will continue to erode.
- His callous and remorseless disregard for the feelings of others means that vulnerable populations will remain at significant risk.
- The typical course for this condition? Deterioration, ending up in a dreary ending for the psychopath, and exhausted and ruined lives for so many of the rest of us.
16
The primary purpose of this essay is to lay out arguments that might help the effort to defeat Trump in the Fall. l suspect that the majority of readers (laypersons and mental health professionals) who have been able to make it through all of the above are like-minded. But I also fret that their reaction might be along the lines of “Duh, obviously [the President is deranged]. Tell me something l don’t know.”
My challenge to that is “No, seriously…”
Seriously, he has a diagnosable condition that “says a lot more” beyond the morass of all his problematic behavior. George Conway, in his excellent article in the Atlantic, “Unfit To Serve”, references Bob Dylan, “You don’t need a weather vane to know to know which way the wind blows,” regarding all of Trump’s misconduct. Perhaps, to know which way the wind blows, but you need more than just a weathervane to know if the wind foretells a benign event, an upcoming thunderstorm, or a tornado. We now have an AccuWeather level of understanding of the man. We know what has hit us and we know what is still barreling toward us.
Seriously, we (mental health professionals) can and should speak with more clarity, precision, uniformity, and authority.
Seriously, we (Democrats and #NeverTrumpers) need to work even harder because the danger is — per his diagnosis — even greater than it appears.
Seriously, the clock is ticking. The Bulletin of the Atomic Scientists — a nonprofit group of scientists and security experts who monitor the possibility of Armageddon caused by humans — has moved the Doomsday Clock 100 seconds to midnight, the closest to midnight the clock has been in its 75-year history. It has moved closer to midnight every year since Trump was elected, except 2019, but only then because they felt “it was a moment in history when fact is becoming indistinguishable from fiction.”
As mental health professionals, we have relevant and substantive insights regarding the President’s mental health. Yet, expert contributions on his psychopathology have not taken hold the way they deserve. What follows is a short list of some of the psychological trap doors that may have compromised our efforts.
II: Why This Article Will Be Ignored
1
This paradox refers to the observation that the more diagnoses we offer for Donald Trump, the less each one registers. In terms of impact on the general public, more is less. Let the Simpson’s creators (i.e., the smartest guys in the room) explain it.
This is what happened in the Goldwater episode. He was tagged with so many diagnoses and (pejorative) psychological descriptors that mental health professionals came across as politically biased and shooting from the hip. No doubt, many sincerely believed he was clinically dangerous. Also, many, no doubt, were gunning to shoot down his candidacy. It is unlikely they had much impact on those voters who were still trying to decide who to vote for.
Since mental health professionals did not do the rigorous diagnostic work, their conclusions about Goldwater were viewed (justifiably) with skepticism. The final impression was along the lines of, “if Goldwater suffers from so many diagnoses, well, really, he probably merits none.” Rather than Goldwater being looked at with suspicion, mental health professionals were.
Ironically and unwittingly, mental health professionals might be replicating a “flooding the zone” phenomenon that has been credited to Trump. A “flooding the zone” occurs when the public (and media) are overwhelmed with so many instances of a trait or misbehavior (in the case of Trump, this involves primarily scandals, violations of democratic norms, gaslighting, etc.) that the impact of any particular trait is diminished. What would have stopped the presses with previous Presidents, doesn’t even make it into the news cycle.
We want to engage the public in a serious argument. But with numerous diagnoses proffered, information overload kicks in and people tune out.
As a side note, in the Dangerous Case and Duty To Warn ( The two key mental health advocacy groups trying to enlighten the public about Trump’s Dangerousness) edited volumes, the following diagnoses and psychological descriptors are put forth by the different contributors: psychotic, paranoid, delusional disorder, grandiose, mania, hypomania, narcissist, malignant narcissist, alpha narcissist, predatory narcissist, psychopath, antisocial disorder, attention deficit disorder, unbridled and extreme present hedonism, dementia, and cognitive decline.
2
The Low-hanging Fruit of Narcissism
Listed above are the many psychiatric diagnoses that have been affixed to Trump. Of these, the diagnosis most often cited vis a vis Trump is Narcissistic Personality Disorder (NPD). When you read the criteria enumerated for NPD in DSM-V, you can understand why:
- Has a grandiose sense of self-importance (e.g., exaggerates achievements and talents, expects to be recognized as superior without commensurate achievements).
- Is preoccupied with fantasies of unlimited success, power, brilliance, beauty, or ideal love.
- Believes that he or she is “special” and unique and can only be understood by, or should associate with, other special or high-status people (or institutions).
- Requires excessive admiration.
- Has a sense of entitlement (i.e., unreasonable expectations of especially favorable treatment or automatic compliance with his or her expectations).
- Is interpersonally exploitative (i.e., takes advantage of others to achieve his or her own ends)
- Lacks empathy: is unwilling to recognize or identify with the feelings or needs of others.
- Is often envious of others or believes that others are envious of him or her.
- Shows arrogant, haughty behaviors or attitudes.
Many of these criteria seem to be written almost with the President in mind. With the thousands of data points available through the archival and informant data, l can say with confidence that Trump meets diagnostic criteria for NPD (please note only five of the nine criteria are needed to warrant the diagnosis).
You may have noticed that some of the traits listed for psychopathy are the same as for Narcissistic Personality Disorder (e.g., grandiose sense of self-worth, lack of empathy, will to dominate and exploit, egocentricity). It is, therefore, not surprising that the comorbidity (the simultaneous presence of two conditions in a patient) between psychopathy and NPD is almost 50%. The two conditions, although meant to convey qualitatively different personality structures, do share a number of traits.
However, to trumpet the diagnosis of NPD for Trump, while technically justified, is misleading and undermines the mission of those of us (e.g. DangerousCase.org) who are trying to fulfill the duty to warn the public. To highlight Trump’s narcissism is misleading because the psychopathic elements of his personality are more central to who he is and how he operates. This can be gleaned from an understanding of the essence of each personality disorder, what psychologists refer to as the deep structure,
As outlined earlier, the deep structure of the psychopath revolves around the core traits of lack of conscience, the drive to dominate relationships because of his inability to care or empathize, and impulsiveness (i.e., the psychopath is a predator without conscience who can’t curb his impulses). The core traits of the narcissist are the excessive need for attention, inflated view of their own importance, and sense of entitlement. There is also general agreement that the narcissist suffers from a fragile self-esteem. This fragility drives him to seek admiration and special treatment, but also leaves him vulnerable to criticism and feelings of low self-esteem when he is not getting his “supply” of approval and applause.
The two disorders share some traits, but their deep structure is different. One is “hot” (the heat of feeling vulnerable) underneath, the other is cold. One is an insecure peacock, the other a snake.
If one examines Trump’s behavior through this deep structured lens, it is evident that his essence is psychopathic. The narcissist breaks rules because he feels special and entitled. The psychopath breaks rules because he wants to secure an advantage. Because of their need for recognition and fear of disapproval, the narcissist will impose certain limits on their behavior. Psychopaths are only concerned about the disapproval of others if it disadvantages them. Their “win at all costs” and lack of conscience results in few limits on their behavior. Narcissists loathe to incur the wrath of others; psychopaths often relish being gleefully evil.
Add to this argument that Trump displays additional traits that are exclusive to the psychopathic diagnosis, such as impulsivity, vindictiveness and history of criminal behavior. The following quote from Trump’s 2004 book, Think Big, flows from a psychopathic rather than narcissistic deep structure state of mind:
I love getting even when l get screwed by someone… Always get even. When you are in business you need to get even with people who screw you. You need to screw them back 15 times harder. You always do it not only to get the person who messed with you but also to show the others who are watching what will happen to them if they screw with you. If someone attacks you, do not hesitate. Go for the jugular.
Psychopathy is a more grave and stringent condition. Yes, narcissists have many problematic traits and can be hell to live with, but they don’t pass the “I would take a bullet to prevent my kid from having this affliction” test (a good thing since the prevalence rate for NPD is 6%). Joe Navarro, a veteran FBI profiler, who authored the book Dangerous Personalities, which examined the combination of different dangerous personalities, characterized the mix of psychopath and narcissist as “Pay attention, as l do what l please.” A clever and apt formulation, but in the case of Trump, should be read as “pay attention, AS I DO WHAT I PLEASE.”
Many with acute myeloid leukemia (AML) develop anemia. It is useful to identify the anemia since it may deserve therapeutic attention in its own right. But no one should think of anemia as on the same ominous plane as AML. Narcissistic Personality Disorder is to psychopathy as anemia is to AML.
Where the two diagnoses diverge is on the issue of dangerousness. The lineup of traits that constitute psychopathy put it in a unique realm of dangerousness. Studies support this assertion. The addition of NPD to diagnostic mix does not, as many have claimed, create a qualitatively different nasty combination, with regard to the level of dangerousness. The lethal mix of traits — the predator like “l can do whatever l please” with remorselessness and on impulse — is contained within the diagnosis of psychopathy.
There is one feature of NPD that applies to Trump and may contribute, at the margins, to his dangerousness. Narcissists are triggered by perceived criticism, which they view as attacks on their self-esteem or status. That can lead to aggressive outbursts and rash decision-making. It is likely Trump gets triggered more often because of this narcissistic vulnerability.
l am suggesting a de-emphasis on Narcissistic Personality Disorder in the psychopolitcal conversation on Trump. Again, he does meet diagnostic criteria for the diagnosis, and it does help explain some of his behavior, particularly his show-stopping, attention-grabbing qualities. However, it does not add significant incremental value to the assessment of dangerousness. I fear so many of us are blinded by the light of his narcissism and theatrics. We need a cutting room session to get beneath that sideshow and to the core of his dangerous psychopathology. The duty to warn compels us.
3
The Allen Frances Criticism and the Construct of “Malignant Narcissism.”
One of the staunchest critics of diagnosing Donald Trump “at a distance” is Allen Frances, a highly respected psychiatrist, who was a chair of the task force to develop DSM-IV.
First, he faults mental health professionals for violating the Goldwater Rule. But, as discussed earlier, the Goldwater Rule has little scientific credibility as a standard in the modern era, particularly when applied to Trump, for whom there is an abundance of life-history and behavioral observation data.
Second, and more critically, he questions whether affixing a diagnosis to Trump adds any important information to what we already know about him. He claims we don’t need to go any further than the observations we already have of his behavior and traits. Psychiatric diagnosis does not provide any useful information beyond its descriptive label and is therefore unproductive.
But this argument appears to be, ipso facto, unreasonable. Of course, a valid diagnosis provides significant surplus information. The diagnosis of psychopathy thru the administration of the PCL-R, enables us to tap into those 3300 studies and make more detailed descriptions of his pathology (e.g., the quality of his lying, the pervasiveness of his impulsivity, the likely brain abnormalities, etc.) and more informed predictions (e.g., about the intractability of his condition, the deteriorating course). And some of the vital information gleamed from the diagnosis is of the non-obvious type.
Allen, certainly no fan of the President, would have us view his behavior as more “bad than mad” (i.e., psychologically disturbed). Without attempting to resolve that epistemological question here, it is obvious that the valid diagnosis of psychopathy in Trump allows us to say “a good deal more” than is conveyed by his “obvious” traits and behavior. Even if we view this constellation of traits as more “bad” than “mad,” it is surely better to have the more extensive and intensive knowledge that the diagnosis affords us. Francis argues for Trump’s removal from office by political means not psychiatric ones. I agree with that. But we can infuse political action with credible diagnostic findings and insights.
Where Frances’ criticism does have merit is in reference to a construct called “malignant narcissism,” which has gained significant traction in the psycho-political conversation on Trump. Malignant narcissism is a construct put forth in 1964 by Erich Fromm, a German social psychologist and Holocaust survivor. It was his attempt to understand some of the monsters of history such as Hitler and Stalin. He characterizes malignant narcissism as “the most severe pathology and the root to the most vicious destructiveness and inhumanity.” ln its current formulation, malignant narcissism is seen as a toxic brew of four personality conditions: paranoid, psychopathic, narcissistic and sadistic.
Donald Trump has been described as a malignant narcissist by a number of mental health professionals, most notably by Dr. John Gartner, the founder of Duty To Warn (www.adutytowarn.org), an organization advocating for the removal of Trump thru the 25th amendment.
But malignant narcissism is not a formal diagnosis. It does not have operationalized criteria. Most critically, it is not tied to a wellspring of studies that provide scientifically validated information on the construct. It very well may be an apt and insightful description of Trump, but — per the Frances criticism — does not add to our knowledge of what we already know about Trump. It is subject to the criticism that it is (however sophisticated) psychiatric “name-calling.” The concern is that “malignant narcissism” has become a shibboleth for those of us who oppose Trump on policy grounds or fear him on psychiatric grounds.
And it is unnecessary.
We run the risk of being seen as nothing but politically biased when we stray from our more scientific role. The diagnosis of psychopathy thru the PCL-R rests on solid empirical ground and, on the score of dangerousness, is damning enough for someone holding the office of the President of the United States. We shouldn’t jeopardize that solid footing by slipping onto the thin ice of hypothetical constructs, no matter how pleasing or on target they seem.
4
We Are Ill-Equipped to Detect and Understand Psychopaths
When it comes to detecting and understanding psychopaths, articles like this are no match for the advantages the psychopath possesses to his “win at all costs” way of being. Robert Hare, the pioneer in the study of psychopathy, felt compelled to step out of his scientific role and issue a warning: “Everyone, including the experts, can be taken in, manipulated, conned and left bewildered by them. A good psychopath can play a concerto on anyone’s heartstrings…Your best defense is to understand the nature of these human predators.”
To provide such an understanding is the purpose of this essay. But l am not optimistic that such an understanding, even if intellectually sound, can hold up against the counterweights aligned against it.
Hare is primarily referring to those traits, the well-honed skills of manipulation, that enable the psychopath to avoid detection. These include the superficial charm, the easy lie, the preternatural ability to portray themselves as victims. Psychopaths rarely present themselves as Hannibal Lectre or Charlie Manson type monsters. More typically, they are charming extroverts who are skilled at impression management. If caught in some immoral or exploitive behavior, they are adept at avoiding responsibility for it, or flipping the script and spinning themselves as deserving of pity.
But these high-level manipulative abilities are not the only or even the main reason psychopaths avoid detection. No, the primary difficulty resides in us, the 99%. Turns out we have evolved in a way that makes it quite difficult to apprehend the presence of psychopathy.
Martha Stout has provided the most insight on this phenomenon, “It is difficult to think of another experience that quite so eludes empathy.” She observes we have no difficulty identifying with and comparing ourselves to others on a wide range of human characteristics, such as states of depression or anxiety, intelligence level, agreeableness, introversion/extroversion and many other personality features.
But not so with psychopathy. Of course, we can recognize instances of immoral or predatory behavior. But we have difficulty comprehending the utter remorselessness that afflicts 1% of us. Stout notes, “But as to what is possibly the single most meaningful characteristic that divides the human species — the presence or absence of conscience — we remain effectively oblivious.”
What might explain this blind spot? Best-selling author Malcolm Gladwell, in his most recent book, Talking to Strangers, highlights a line of research that seems pertinent. He was exploring the problem of why we are so poor at identifying bad actors in our midst — spies, financial con men, sexual predators, prisoners that are poor bail risks. While in some cases this represents the “skill” of the psychopath, it also holds true when there are many clues available that should have raised suspicions. We (and this certainly includes trained professionals) are particularly bad at forming accurate judgements of bad guys.
To provide insight into this phenomenon, Gladwell cites the “default to truth” theory developed by a psychologist at the University of Alabama, Tim Levine. Levine’s studies and theories are presented in his book, Duped: Truth-Default Theory and the Social Science of Lying and Deception. In a range of clever studies, Levine demonstrated that when there are many clues that a stranger is lying, we nevertheless default to assuming he is telling the truth. Default to truth is our baseline assumption and we stubbornly hold onto it unless our doubts reach such a level that they can’t be explained away.
Gladwell points to the Larry Nassar sex abuse scandal as a dark example of this theory. Nassar was a doctor at Michigan State and the team physician for the USA gymnastics women’s national team. He abused hundreds of young female athletes. He did so in an obvious, overt manner, although he framed his behavior as medical treatment. Still, the situation, looking back on it, was obvious. Yet, it went on for years.
The reason for this travesty of accountability was not some kind of coverup by authorities, but default to truth. Not only were authorities reluctant to believe accusations brought against Nassar, but court records show many young women and their parents, although suspicious, were also reluctant to believe that a health care professional with an unassuming style was delivering anything other than what he professed was appropriate medical treatment.
Levine notes the default to truth mindset is particularly strong when one is faced with two alternative interpretations, where one is plausible (e.g., see the Establishment Republican meme: “He’s just a different kind of President”) and the other is impossible to accept (he just might have a condition where he “carries disaster lightly in both hands”). The default to truth tendency seems to represent not so much a lack of judgement as the way our brains are wired.
The default to truth mode may help describe our blind spot, but what explains having such a blind spot? Elizabeth Stout believes the answer lies in evolutionary theory, specifically the proposition that the unit for the natural selection of genes is the group rather than the individual. Genes that get selected and thus shape human nature over time are ones that favor survival of the group. Thus, genes selected are ones that promote bonding, trust, unselfishness and peace. And, most assuredly, a conscience, which flows from the sense of obligation based on attachment to others.
The group theory of gene selection was first advanced by Richard Dawkins in his book, The Selfish Gene. As a side note, this title is somewhat ironic. Dawkins was saying genes associated with unselfish behavior were privileged over genes associated with selfish behavior, and thus could be considered “selfish” in the sense of advancing their interest of group survival). If the unit of genetic selection were the individual, then genes associated with ‘looking out for number one’ would be privileged. Selfishness and remorselessness would serve as advantages to the individual in the survival of the fittest race but would be destabilizing and eventually disastrous to the group (feel free to substitute the words Trump and USA for the words individual and group).
Of course, we all live the struggle between our selfish impulses (what’s good for us) and our more altruistic ones (what’s good for our loved ones and the greater community). But, overall, we seemed to have evolved as (far from perfect) moral, truth-telling, unselfish animals. Among other qualities, that has left us with a great difficulty in detecting or even imagining that 1% of us are remorseless and can live, with predatory calculation, totally outside the human contract.
And that one of that 1% now sits in the Oval Office.
There are other psychological forces that pose barriers to getting the message thru on Trump’s mental health. At this point there is a robust literature on the tribal sentiments and passions that undergird his support. Arguments based on rationality and scientific empiricism are associated with Blue Tribe elites and therefore are repugnant for those in the Red Tribe.
Finally, there appears to be a large swab of the electorate who are drawn to nihilism and chaos (see Thomas Edsall’s “The Trump Voters Whose Need for Chaos Obliterates Everything Else,” New York Times — 9/04/19). In our upside-down current predicament, this makes his divisive and destructive behavior attractive to many voters.
We can only hope that our awareness of these counterintuitive variables will enable us to find more creative ways to get our message across.
5
Of course, although I hypothesize why this article might be ignored, l hope it will not and may even help in the effort to defeat Trump. In that spirit, I make the following pleas:
To undecided voters:
Appreciate your consideration of the material in this essay. Perhaps a few of you have been swayed by it. Perhaps a few of you, understandably exhausted and discouraged by our political circus, will nevertheless push yourselves to come out and vote.
To “Influencers:” -In the mainstream media, in your writings and broadcasts, you no longer have to refer to Trump as an “undiagnosed” psychopath (or sociopath). He has now been diagnosed with an instrument of impressive validity. Also, when you are wanting to describe him as a “different kind of President,” you are encouraged to articulate the particular traits he is displaying, and place them in the context of his broader pathological condition.
- In social media, Would certainly appreciate however many clicks you can bring to this article.
To activists and NeverTrumpers:
Thank you for your work. Most analyses emphasize this is to be a turnout election, which highlights the role of getting out the vote. Hoping this article supports your efforts to knock on even a few more doors, to ask for or contribute a bit more money.
And, most of all…
To my mental health colleagues -
I hope this essay has demonstrated we stand on firm empirical ground; and can and should speak with authority to the President’s psychopathology. If you think the arguments put forth in this essay have merit, then l would suggest that we prioritize the message that Trump meets strict criteria for clinical psychopathy. The reason, as noted in the “Mr. Burns Paradox” above, is that heralding so many diagnoses for him dilutes our message to laypersons. We have expertise concerning this personality disorder. We know that Trump’s behavior doesn’t just “speak for itself” but reveals an underlying pathology that is clearly delineated and ominous. Coalescing around the primary diagnosis of psychopathy underscores his dangerousness and strengthens our message.
We need to Paul Revere that message.
November is coming, November is coming…
— — — — — — — — — — — — — — — — — — — — — — — — — — — — -
Notes
page 9 - For a more thorough discussion of the Hare Psychopathy Checklist see Hare. R.D. Without Conscience: The Disturbing World of the Psychopaths Among Us. New York: Guilford Press, 1998.
page 12-The empirical strength of the Hare Psychopathy Checklist is examined in The Clinical and Forensic Assessment of Psychopathy, A Practitioner’s Guide. This is the go-to book for those interested in the research and practice on the assessment of psychopathy. The volume has chapters on the brain imaging work with psychopaths, as well as other characteristics that undergird the validity of the construct. Most critically, it contains scholarly reviews and analysis of the clinical use of the Hare Psychopathy Checklist.
page 14- M. Lyons et. al. “Differential Heritability of Adult and Juvenile Antisocial Traits,” Archives of General Psychiatry 52 (1995): 906–915.
page 14 -The Texas Adoption Project: See L. Willerman, J, Loehlin and J. Horn, “An Adoption and Cross-Fostering Study of the MMPI Psychopathic Deviate Scale,” Behavior Genetics, 22 (1992): 515–529.
page 14- “A different brain is the short answer.” In 2008, John Seabrook wrote an article in the New Yorker titled Suffering Souls: The Search for the Roots of Psychopathy. It is largely a profile of Dr. Kent Kiehl, the leading expert on brain imaging and psychopathy.
page 17- “An existence unmolested by the rumblings of a soul,” From a profile by Mark Singer also in the New Yorker.
page 18- Executioner’s Song won the Pulitzer Prize in1980. Mailer uses non-fiction craft elements to capture the coldness and remorselessness of the psychopath.
page 21- Neurotic Styles by David Shapiro. For mental health professionals ‘of a certain age’, this was a revelatory textbook which delineated the inner life of various psychopathological states.
page 33- George Conway does as thorough a job as a layman can of examining Trump’s behavior through the prism of DSM-V.
page 37- Allen Frances has been one of the most forceful and insightful critics of Trump(see especially Twilight of American Sanity). He delineates Trump’s destructive personality traits and their ruinous impact on the world. We simply disagree on the incremental value a formal diagnosis of psychopathy provides.
page 39 Gladwell explores a number of ways we can misjudge others across different contexts. The ‘default to truth’ findings are just one factor contributing to our difficulty in detecting psychopaths.
page 40- “robust literature on tribal sentiments”, see especially Francis Fukuyama, Identi ty: The Demand for Dignity and the Politics of Resentment, and Ezra Klein, WhyWe’re Polarized.
Please note: This article is not financed by or related to any political campaign and may not be considered political advertising or action on behalf of any political candidate. All statements and opinions are those of the author alone, including any political endorsements made. The information published in this article is for information only and is not intended to provide psychological therapy or diagnostic advice and/or recommendations to any persons aside from its subject, Donald J. Trump, a public figure. The content of this article is intended to provide informational, scientific and educational material based on psychological science. The content of this article solely reflects the views and perspectives of its author and does not necessarily reflect the views or positions of the American Psychological Association, medium.com, or any other person and/or entity not otherwise listed as an author.
