Does Donald Trump Show Signs of Neurodegenerative Disease?

The data suggests he does and the implications are serious.
by Vincent Greenwood, Ph.D., founder of DutyToInform.org
What would it mean if Donald Trump (or any candidate seeking higher office, for that matter) were suffering from a deteriorating neurological syndrome rather than just the typical vicissitudes of aging? The mild decline in memory, attention, and verbal fluency associated with normal aging often emerges as one reaches their late 70s or early 80s. Such decline would not necessarily be disqualifying, even regarding the demanding responsibilities of the presidency. However, a diagnosis of a deteriorating neurological disorder would have profound implications for their fitness for office. If the ex-president crossed that fateful diagnostic threshold, the public would have a right to be informed and a reason to be alarmed.
Although many observers, including healthcare professionals, have commented on Donald Trump’s verbal and cognitive struggles over the past couple of years, conventional wisdom has concluded that it is simply not possible to make a valid diagnosis of neurological decline with Trump. Many good faith investigative reporters and health care professionals cite two reasons why we are not able to diagnose the possibility of a neurological disorder: the lack of medical information released by Trump and his doctors; and the inherent limitations of ‘diagnosing at a distance,’ which is the only resort available since Trump has refused to undergo a comprehensive neuropsychological examination.
These are reasonable objections that need to be addressed. The frustration over Trump’s refusal to release detailed health information is captured in a recent article by investigative journalists at the New York Times titled What Are We Told About the Health of Biden and Trump? They Decide. Trump and his medical team have gone out of their way in not providing detailed information. His most recent report (November 2023) is a three-paragraph statement where his physician described his health as “excellent.” Earlier health reports have been criticized as “fawning and vague,” marked by the use of superlatives (“the healthiest individual ever elected to the presidency”), and lack of details.
And full of disinformation. Here, we need to mention Trump’s assertions about a “cognitive test” he took in 2018, the Montreal Cognitive Assessment Test (MoCA). The MoCa, a one-page, 30-point test that can be administered in 10 minutes, is an initial screening device that can detect signs of full-scale dementia. It is not particularly helpful in identifying signs of early dementia, which requires much more rigorous and lengthy testing. Trump reported a perfect score of 30, claiming doctors told him that “rarely can anybody do what you just did” and that the test contains “very hard” questions. The average score on the test is 27 (and even that average is taken from a sample of people suspected of cognitive impairment). A score of 30 is considered normal, not exceptional. Examples of questions from the supposedly tricky part of the test include repeating a sentence out loud, naming as many words as you can starting with the letter F, trying to identify the similarity between different objects such as trains and bicycles (modes of transportation), and saying what the current date is. Dr. Jonathan Reiner, professor of Medicine and Surgery at George Washington Hospital, wryly observed, “If you think a dementia screening test is very difficult, you may have early dementia.”
We are not able to make a serious appraisal of whether Trump does or does not display brain illness based on his released medical records since they lack any specificity and have been politicized.
Since Trump has refused to collaborate in a comprehensive neuropsychological exam, which would yield a wealth of relevant data, we must rely on ‘diagnosing at a distance’ to try to determine the possibility of meaningful cognitive decline. The limitations of such an approach are outlined in a recent Washington Post article, What Science Tells Us about Biden, Trump and Evaluating an Aging Brain. Experts interviewed for that story assert that an informed opinion on the ex-president’s cognitive health is only possible with the robust data generated from an in-depth exam. They note, correctly, that video mashups of verbal gaffes lack scientific rigor and can be misleading. These video mashups on social media can be guilty of cherry-picking bad moments and equating signs of normal aging with severe cognitive decline.
Are we forced to throw up our hands with the possibility of providing a more scientific and objective opinion about whether Trump suffers from a neurocognitive disorder?
The answer is no. There is a legitimate path to arrive at an informed, scientifically-based opinion on Trump’s brain health. That path involves subjecting all the relevant information to the guidelines enumerated in the chapter on Neurocognitive Disorders in the latest version of the Diagnostic and Statistical Manual of Mental Disorders. When we carry out those diagnostic steps, we find that Trump very likely has a Neurocognitive Disorder that is already beginning to have its way with his cognitive functioning and is destined to deteriorate, perhaps significantly, over the next few years.
With all its implications, such a serious assertion demands a serious explanation. Let’s start with the scientific standing of the diagnostic bible of the mental health profession. The Diagnostic and Statistical Manual of Mental Disorders — Version 5 (DSM-5), the authoritative and up-to-date (latest revision in 2022) resource that provides a unified classification of mental health and brain-related conditions. DSM-5 offers a common framework and language to define primary psychopathological syndromes and then provides specific criteria to diagnose them.
The manual organizes those conditions into chapters that focus on distinct groups of disorders. Neurological disorders, including dementia, are discussed in the Neurocognitive Disorders chapter. Neurocognitive Disorder is a general term that describes decreased cognitive functioning due to a medical disease other than a psychiatric illness. The authors of the Neurocognitive Disorders chapter in DSM-5 included some of the globe’s leading experts in geriatric psychiatry, neurology, neuropsychology, and psychiatric research. This group of experts (The Neurocognitive Disorders Work Group) spent five years evaluating the latest advances in scientific knowledge and honing the definitions of neurological conditions. From that effort, they distilled the broad array of neurological difficulties and the various brain illnesses that can produce those difficulties, such as Alzheimer’s or cerebrovascular disease, into three primary syndromes, three basic Neurocognitive Disorders (NCDs).
The three basic syndromes or primary diagnoses are Delirium, Mild Neurocognitive Disorder, and Major Neurocognitive Disorder.
Delirium is an altered state of consciousness in which the patient is confused, disoriented, and unable to think or remember clearly. It comes rapidly, usually within hours or days, and is treatable, especially if the diagnostician can identify the underlying cause. There is no particular concern that Trump suffers from delirium.
Nor is there concern that Trump meets the diagnostic criteria for Major Neurocognitive Disorder at the present moment. Major NCD is the syndrome we associate with full-scale dementia where there is a dramatic loss of capacities that undermines one’s ability to live independently.
This leaves the syndrome of Mild Neurocognitive Disorder — what we think of as likely early dementia — as the condition that might explain Trump’s recent struggles. In Mild NCD, independent living continues, but the person displays moderate decline and signs of struggle in one or more essential areas of functioning.
To determine if Donald Trump displays Mild NCD, we need to look at the DSM-5 criteria for this diagnosis. The diagnosis of a Neurocognitive Disorder is all about the decline in a critical area of human functioning, referred to as cognitive domains in DSM-5. The diagnostician is looking for decline across six such domains, which are:
Attention
Memory
Language
Executive Functioning
Perceptual-Motor
Social Cognition
The authors of the Neurocognitive Disorder Chapter determined that if you can demonstrate a decline in even just one of these domains, you must consider a diagnosis of one of the neurocognitive syndromes. If the decline is “substantial” and the struggle with independent living is significant, the diagnosis of Major NCD (full-blown) dementia is warranted. If the decline is “moderate” and the struggle with independent living is just beginning to emerge, a diagnosis of Mild NCD is justified.
If there is concern one might be in the throes of a Neurocognitive Disorder, you would undertake a comprehensive assessment of these domains. The gold standard of such an evaluation would involve administering fine-grained neuropsychological tests in each domain. This is where frustration over Trump’s refusal to release details of his medical exams or collaborate in such testing is felt.
However, even without this cooperation, there are two other sources of potentially relevant information: (1) reports from biographers or close observers of Trump and (2) direct observation of his behavior in these domains.
What can we glean from these sources vis-a-vis the six key cognitive domains?
Information from close observers — colleagues, employees, family, friends, journalists, such as Tony Schwartz, co-author of The Art of the Deal — and well-sourced biographies is beneficial in assessing executive functioning, attention, and social cognition. These domains consist of a broad swath of behavior, much of it occurring off-camera. To get a decent appraisal, one must assess these behaviors over many situations and months, if not years.
From these many insider accounts and biographies, we have copious evidence that Trump’s functioning in these areas is markedly below average. He has a notoriously short attention span; disdains the planning, focus on details, and self-control that comprise executive functioning; and has a lifelong history of disagreeableness and lack of empathy that are at the heart of competent social cognition.
However, it seems hard to argue that Trump’s struggles in these areas are a result of a neurodegenerative disease process. Remember, diagnosing a Neurocognitive Disorder requires the demonstration of decline in one or more of the six cognitive domains. A comprehensive review of Trump’s biographies reveals persistent deficiencies in attention, executive functioning, and social cognition dating back to childhood and quite prominent in his middle age.
Still, thanks to reams of videotape on Trump, we have access to many behavioral observations to evaluate for possible cognitive decline. Direct behavioral observation is particularly relevant for the domains of memory, perceptual-motor skills (how one can navigate the world physically), and language.
Trump occasionally mixes up people — Nikki Haley for Nancy Pelosi, mayor Willie Brown for a councilman are recent examples — rather than just names. This confusion can be a sign of cognitive decline in the memory domain. Trump’s bent, forward-listing posture, jerking right arm and leg, and arm weakness are also worrisome signs of neurological dysfunction and not just normal aging. However, while there are several red flags of neurological issues for Trump in the areas of memory and perceptual-motor skills, there is not sufficient evidence to give a definitive diagnosis of Neurocognitive Disorder.
This leaves us with one domain to evaluate such a possibility: language. Fortunately, this domain does not require collaboration with Trump. That’s because you can execute a detailed, clinically meaningful appraisal directly from speech samples, which are readily available on YouTube. Furthermore, you can zero in on possible decline in the language domain by comparing speech samples from the past to the present.
To measure decline more rigorously, we developed the following checklist of seven specific verbal expressive behaviors that have been linked to neurodegenerative brain illness.
Table 1: Verbal Markers Linked To Neurocognitive Disorder
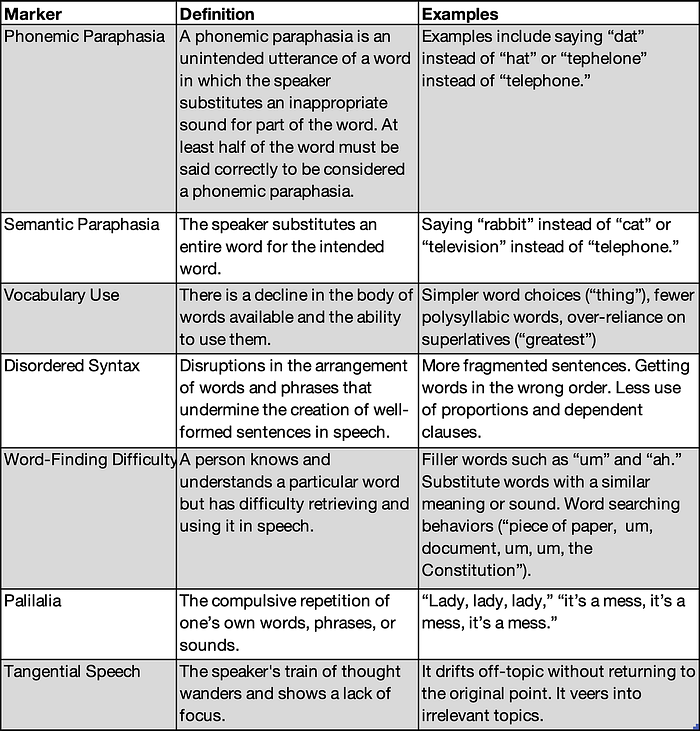
Because of their specificity, these markers allow for a more objective determination of cognitive decline in the language domain. Because of their empirical support, they allow for a more valid determination of clinically meaningful decline.
We then applied the checklist to randomly selected speech samples of Trump from his middle age and recent past. Trump displayed shifts in all seven markers. He received ratings of “never” or “rarely” for all markers from the years 1975–2000 versus “moderately” or “frequently” for all markers from the years 2020 — present. I also developed a list of seven specific verbal expressive behaviors associated with normal aging, such as speech volume and rate. I applied that checklist to the same Trump speech samples. For a man of his age, Trump actually displays minimal signs of aging in his verbal expressive behavior.
Thus, Trump shows clinically significant signs of cognitive decline in the language domain beyond normal aging.
The findings outlined above are reinforced by other studies that have examined Trump’s language behavior. In Trump Wasn’t Always So Linguistically Challenged-What Could Explain The Change? Begley noted “striking and unmistakable” shifts In his vocabulary level and ability to string sentences together. In Popular Press Claims Regarding Linguistic Change in President Donald J. Trump, a study that zeroed in on word-finding difficulties, investigators found Trump displayed a “systematic increase in the use of filler words.” The author of a recent study that applied a metric of analytic thinking to Trump’s contemporary speeches concluded, “I can’t tell you how staggering this is. He does not think in a complex way at all.” STAT, a media organization focused on health research, asked experts in memory, psychology, and linguistics to compare clips of Trump’s speech from 2017 to clips from 2024. They concluded that “Trump’s speech included more short sentences, a confused order of words, repetition and extended digressions.”
We now have accumulating evidence that Donald Trump displays a meaningful decline in language functioning. Language functioning is one of the six key cognitive domains cited in DSM-5, where a moderate decline in functioning is sufficient to trigger a formal diagnosis of Mild Neurocognitive Disorder, a condition associated with underlying brain disease.
The implications of this diagnosis are sobering when one considers the responsibilities of the presidency. First, if Trump is showing meaningful decline in one cognitive domain, it is likely that troubles are beginning to emerge in the other areas of functioning. What might this look like in practical terms? Here are some examples:
· Attention — tasks take longer to complete than previously, and work must be double-checked for errors.
· Executive functioning — requires more effort to finish multistep projects, has trouble resuming an interrupted task, and has difficulty organizing, planning, or making decisions.
· Learning and memory — difficulty recalling recent events, relies on reminders and list-making.
· Perceptual-motor skills — may rely more heavily on maps or notes for directions.
· Social cognition — less ability to read social cues, such as facial expressions, decreased empathy, or decreased inhibition.
Second, and most critically, this condition almost always progresses to full-scale dementia. How fast? Studies indicate that just within one year, 15 percent or even 20 percent of those with Mild NCD will develop full-scale dementia (Major NCD). That percentage, called the annual conversion rate, applies to successive years, thus increasing the risk of full-scale dementia over time, rising to over 50% within four years.
Another risk factor for Trump is the fact his father, Fred, was diagnosed with Alzheimer’s. Individuals with a first-degree relative, such as a parent, who had Alzheimer’s, are more likely to develop the condition — their risk increases by about 30 percent. Scientists have identified a gene variant, called apolipoprotein4 (APOE4), that increases your risk three times beyond that. Testing for the gene is safe, straightforward, and inexpensive. I could not find anywhere in his reported health records that Trump had submitted to that genetic test.
Given the evidence of likely neurodegenerative illness, I would like to make a plea to the ex-President:
It might be frightening to undergo a comprehensive neuropsychological workup or genetic testing. Taking such a step is typically considered a personal choice and a protected right for any individual. However, a core value in a democracy is an informed citizenry. Citizens have a right to information that is relevant and meaningful for those seeking office for positions that affect the general welfare. This duty to inform would include, but not be limited to, considerations of dangerousness.
As difficult as it might be, you have a moral duty to inform the public about the distinct possibility that you might be in the beginning stage of a deteriorating neurological disorder. Sir, please do the right thing and collaborate on a comprehensive neuropsychological exam.
Please note: This article is not financed by or related to any political campaign and may not be considered political advertising or action on behalf of any political candidate. All statements and opinions are those of the author alone, including any political endorsements made. The information published in this article is for information only and is not intended to provide psychological therapy or diagnostic advice and/or recommendations to any persons aside from its subject, Donald J. Trump, public figure. The content of this article is intended to provide informational, scientific, and educational material based on psychological science. The content of this article solely reflects the views and perspectives of its author and does not necessarily reflect the views or positions of the American Psychological Association, medium.com, or any other person and/or entity not otherwise listed as an author.
