DUTY TO INFORM (PART 1)
Does Trump or Biden Display Neurocognitive Disorder? Where We Stand Now

A Cautious Appraisal Still Yields Concern About One Of Our Candidates
Over the past few years, there has been increasing conjecture over whether President Biden might be in an early stage of dementia (Please note: the term Major Neurocognitive Disorder (NCD) has replaced the term dementia in the most recent version of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), the authoritative guide for diagnosing mental disorders. The terms are interchangeable, and we use both in this article). On Fox News and other right-wing outlets, Biden’s unfitness for office due to this supposed neurological deterioration is a given and is reinforced by (creative) video mashups highlighting his verbal disfluencies. And this characterization is not just on Fox News. Mainstream media — the New York Times is one example — has increasingly focused on Biden’s age and its implications for his mental capacities.
More recently, we see the same concern about Trump. Mashups of his verbal slip-ups have emerged. More substantively, experts from the fields of clinical neurology and psychology have weighed in on the peculiar quality of Trump’s linguistic and cognitive struggles, noting that his observed difficulties seem to indicate a disease process of neurological decline rather than normal aging. Recent findings have been collated and critiqued by John Gartner, founder of Duty To Warn, and summarized in a petition signed to date by over 2,000 healthcare professionals. These trained clinicians are troubled, if not alarmed, by Trump’s neurological state.
The alarm is well-founded. If either Biden or Trump were displaying signs that they were in the beginning stage of a degenerative brain disease rather than just signs of normal aging, it would have profound implications for their fitness for office. Their ability to handle the responsibilities of the office as well as their ability to ward off further deterioration of their neurological condition would be seriously compromised.
Of course, both candidates deny any suggestion that they suffer from cognitive decline and cite recent medical examinations to back up their assertions of cognitive health. Yet doubts about their cognitive health remain throughout the country. These doubts are exacerbated by what they hear from pundits and, more recently, health care professionals. But also, understandably, by what they see and hear with their own eyes and ears.
Is having a more scientific and informed opinion about Biden and Trump’s brain health possible? Do we have to rely only on dueling video mashups? This paper aims to take advantage of scientifically-based knowledge about neurodegenerative
disorders and applies differential diagnosis tools to see if some objectivity can be injected into this critical conversation. Even though we do not benefit from their collaboration in a comprehensive diagnostic workup, I hope to demonstrate that we can nevertheless make substantive assertions about Biden and Trump’s cognitive status.
DSM-5 Definitions and Diagnostic Criteria for Neurocognitive Disorders
DSM-5 is the authoritative and up-to-date resource that provides a unified classification of mental disorders and is the best place to seek insight on the assertions about Biden and Trump’s cognitive health. DSM-5 offers a common framework and language to define primary psychopathological syndromes and then provides specific criteria to diagnose them. Conforming to the guidelines in the Neurocognitive Disorder (NCD) chapter of DSM-5 can take us beyond the realm of speculation, beyond even well-intentioned and well-informed clinical opinions, and onto firmer scientific ground that has been seeded by the leading international experts in clinical neurology, who used the latest advances in scientific knowledge in the field to produce the chapter on neurological disorders in DSM-5. This expert working group on these disorders took five years to hone these definitions and diagnostic criteria for the latest version of our diagnostic manual. It achieved notable inroads in our understanding of and ability to diagnose NCDs reliably.
A synopsis of these definitions and diagnostic criteria is necessary to provide context to our assertions about Biden and Trump’s brain health.
DSM-5 provides detailed definitions of mental health and brain-related conditions. The manual organizes those conditions into chapters that focus on distinct groups of disorders. Neurological disorders, including dementia, are discussed in the Neurocognitive Disorders (NCDs) chapter. The chapter title “Neurocognitive Disorders” is a change from the DSM-4 version of the manual, where the chapter on neurological conditions was titled “Delirium, Dementia, and Amnestic and Other Cognitive Disorders.” The developers of DSM-5 changed the name to reduce the negative stigma associated with the word dementia, whose original meaning came from the word “demens,” which means “without mind.”
[I would also add that recently, the word dementia has been thrown around a good deal, particularly in social media. As I hope it will become apparent in this article, it is essential to use the terms “dementia” or “early dementia” in a strictly scientific and diagnostic sense and not just as a descriptor of troubling cognitive or verbal behaviors. (On Fox News, they often use the term senile about Biden, which is considered even more disparaging).]
In this paper, we address the question of whether Biden or Trump warrant serious consideration for a Neurocognitive Disorder, specifically early or full-scale dementia as defined in DSM-5. To try to answer that question, we begin with the DSM-5 definition of a Neurocognitive Disorder, highlighting the two most fundamental features of these disorders (italics for emphasis are mine).
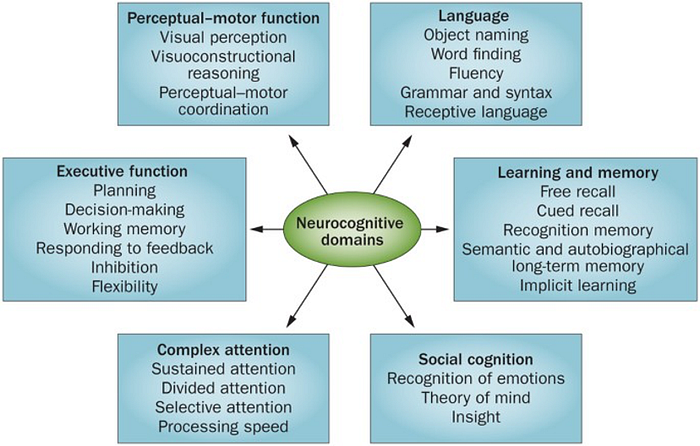
First, Neurocognitive disorder (NCD) is a general term that describes decreased cognitive functioning due to a medical disease other than a psychiatric illness. Diagnosis of NCD is all about cognitive decline from a previous, healthier baseline. The essential data for diagnosing NCDs is based on performance in six cognitive domains: complex attention, executive functioning, learning and memory, language, perceptual-motor abilities, and social cognition. The diagnostician’s task is to measure the possible decline in these six and only these six domains. The manual contains definitions and examples of decline for each of these domains.
Second, the Neurocognitive Disorders category consists of three primary syndromes: Delirium, Mild Neurocognitive Disorder, and Major Neurocognitive Disorder. These are the three and only three primary diagnoses in this category.
DSM-5, compared to earlier versions of the manual, has brought cohesion to the broad array of neurological difficulties by synthesizing the diagnostic field to just these three syndromes. They accomplished this by disentangling the consequences of neurological disorders (the three primary syndromes/diagnoses) from their causes. The causes or etiologies are usually illnesses, such as Alzheimer’s or cerebrovascular disease, or insults to the brain, such as concussion or substance abuse. Suppose a patient warrants a diagnosis of one of the three syndromes. In that case, the diagnostician is asked to identify the cause, which is then listed as a subtype of the primary diagnosis. A list of the most frequently occurring etiologies is in the appendix.
Again, please note the term “dementia” or “full-scale dementia” is now synonymous with the term “Major Neurocognitive Disorder.” The term “early dementia” should be used only in reference to Mild NCD.
[One of the three syndromes, delirium, is irrelevant to the Biden/Trump conversation. Delirium is an altered state of consciousness in which the patient is confused, disoriented, and unable to think or remember clearly. It comes on rapidly, usually within hours or days, and is treatable, especially if the diagnostician can identify the underlying cause. There is no concern that Biden or Trump suffer from delirium.]
Now that we have a precise definition of Neurocognitive Disorder, we can turn to the diagnostic criteria and guidelines that allow us to determine whether a particular person has one of the three basic syndromes.
The full diagnostic criteria for the three syndromes, as laid out in DSM-5, are in the appendix. However, the “Cliff Notes” diagnostic algorithm is as follows:
(1) Assess the six cognitive domains — complex attention, executive functioning, learning and memory, language, perceptual-motor abilities, and social cognition — and determine if there has been a noticeable decline in at least one. If there is, you have established there is a diagnosable Neurocognitive disorder. (You do need to make sure the decline is not better explained by another mental disorder, such as schizophrenia or major depression.)
(2) Assess whether the decline is “substantial” or “modest” and whether the impact on independent living is significant or very mild. These distinctions enable you to determine if the diagnosis is Major NCD or Mild NCD. With Major Neurocognitive Disorder (dementia), there is a “significant” decline in cognitive functioning, whereas with Mild Neurocognitive Disorder (possible early dementia), there is a “modest” decline. In Major Neurocognitive Disorder (dementia), the cognitive deficits “interfere with independence in daily activities’ (e.g., on the mild end, this means activities such as paying bills and managing medication, and on the severe end, activities such as dressing, toileting, and eating). In Mild Neurocognitive Disorder (possible early dementia), there is no significant interference with independence in daily living. However, struggle and compensatory strategies (e.g., making lists and using pill boxes) are emerging to maintain independent living.
(3) If the diagnostic criteria for one of the three syndromes are met, then the diagnostician is tasked to identify “possible or probable subtypes,” such as Alzheimer’s disease. Please note that it is not necessary to identify the etiological subtype to diagnose a Neurocognitive Disorder. With Mild NCD, we usually cannot identify the underlying cause of the neural disruption. Not being able to locate the cause of the NCD syndrome in no way detracts from the validity of the primary diagnosis. For a graphic explaining this breakdown, visit this link.
As you can see, the diagnostic guidelines to determine whether one has a Neurocognitive Disorder are straightforward and efficient. They have been developed to achieve the best reliability and validity metrics. That does not mean it is easy to earn such a diagnosis. It is a fateful diagnosis with profound implications.
If these trustworthy diagnostic criteria for Biden or Trump are not met, then the explanation of neurological dysfunction for their recent behavior that concerns so many is discredited. Of course, if those concerns are discredited, other answers for such behavior can be sought, such as normal aging, Biden’s diagnosed stuttering problem, or Trump’s possible other psychiatric vulnerabilities. But you would first have to rule out neurological dysfunction. That is, assuming you give deference to the authors of DSM-5, some of the leading experts in the world on brain-related conditions and whose diagnostic categories rest on an empirical foundation of all pertinent research to date.
The ability to confidently diagnose Neurocognitive Disorder, whether from a personal examination or from a distance, will revolve around the quantity and relevance of the available data. We will get to the data shortly, but first we need to consider how consequential a diagnosis of one of the Neurocognitive Disorder syndromes would be for someone running for the presidency of the United States.
As noted above, we don’t need to delve into what it means to suffer from Delirium. Instead, we need to consider the ramifications of meeting diagnostic criteria for Mild Neurocognitive Disorder (likely early dementia) or Major Neurocognitive Disorder (full-scale dementia)?
Implications of Receiving a Diagnosis of Mild Neurocognitive Disorder (Likely Early Dementia)
Don’t let the word “mild” mislead you.
To warrant this diagnosis, you must show a moderate decline from a previous level of performance in one of the six cognitive domains as noted above and in the DSM-5. What might this mean in practical terms? Here are some examples:
· Attention — tasks take longer to complete than they did previously, and work needs to be double-checked for errors.
· Executive functioning — requires more effort to finish multistep projects, trouble resuming a task that was interrupted, and has difficulty organizing, planning, or making decisions.
· Learning and memory — difficulty recalling recent events, relies on reminders and list-making.
· Language — word-finding difficulty, grammatical errors in expressive language.
· Perceptual-motor skills — may rely more heavily on maps or notes for directions.
· Social cognition — less ability to read social cues, such as facial expressions, decreased empathy, or decreased inhibition.
You only need a moderate decline in one of these areas to be considered for the diagnosis. The reason for needing to show a decline in only one of the six cognitive domains to warrant a diagnosis of Mild NCD deserves an explanation. As of yet, we do not have reliable biomarkers (a biological molecule found in blood, other body fluids, or tissues that are a sign of an abnormal process or disease) of early dementia. However, the authors of the Neurocognitive Disorders Chapter of the DSM-5 determined that evidence of decline in any one of the six cognitive domains was a strong indicator of underlying neural disruption and justified the diagnosis. Each of these domains represents a critical area of human functioning, and the meaningful decline of any one is ominous. Moderate cognitive decline is the empirical gold that neuro-diagnosticians are panning for with this diagnosis.
While these midsize declines in cognitive functioning don’t yet undermine the capacity for independent living, we see the emergence of “effort, compensatory strategies, and accommodations” (from the DSM-5 criteria for Mild NCD) to maintain that independent living. This struggle to preserve independence is often played out in instrumental activities of daily living (IADLs). IADLs are things you do every day to take care of yourself and manage your home and life. Examples include preparing meals, performing household chores and repairs, driving or using public transportation, shopping for clothes or food, and handling your finances. While these instrumental activities might not be relevant to the unique and privileged lifestyles of Biden and Trump, with this diagnosis, you would start to see accommodations in their relevant daily routines that had once been routine and performed with ease.
When someone is given this diagnosis, it is often a time when family and loved ones begin the sober appraisal of whether the individual might need more protection and surveillance, or begin to consider the option of assisted living if the condition deteriorates. Such concerns are well-founded when we turn to the most significant aspect of this condition: its course or prognosis.
What is the fate of someone once they cross the diagnostic threshold for Mild NCD? Fortunately, a few recover and reverse their cognitive decline. This reversal occurs when an underlying cause — other than brain disease — is identified. The main nonbrain disease culprits that can evoke the symptoms of Mild NCD are side effects of medications that can cause confusion, infections, sight or hearing loss, alcohol abuse, and major clinical depression. These conditions are treatable, and once treated, the symptoms of Mild NCD get better or even go away with time.
It should be noted that nothing in their health records suggest Biden or Trump has dealt seriously with any of these modifiable conditions that could lead to Mild NCD. And, of course, they have access to top-flight medical attention that would likely prevent or quickly detect and treat these conditions. Thus, a diagnosis of Mild Neurocognitive Disorder for either of them would strongly suggest the early stages of a neurodegenerative illness.
Most individuals with Mild NCD develop more severe neurological dysfunction over time, eventually leading to a diagnosis of Major NCD (dementia) that carries with it the loss of the capacity for independent living. How fast does this happen once you receive a diagnosis of Mild NCD? Pretty fast.
Studies indicate that just within one year, 15 percent or even 20 percent of those with Mild NCD will develop full-scale dementia (Major NCD). That percentage, called the annual conversion rate, applies to successive years, thus increasing the risk of dementia over time. Therefore, hypothetically, if one of our candidates were diagnosed right now with Mild NCD, there would be around an 8% chance of full-scale dementia by Inauguration Day, with the risk rising to around 20%-25% one year into his term. Given the tremendous burden and stakes associated with the presidency, the scientific term for such risk would be “Yikes!”
Don’t let the world “mild” mislead you
Implications of Receiving a Diagnosis of Major Neurocognitive Disorder (Dementia)
Major NCD is characterized by a persistent worsening in cognitive functioning and a loss of capacity to do daily tasks. Hypothetically, if we believed this diagnosis was valid for someone sitting in the Oval Office or running for it, the scientific term for that predicament would be “game over.” The most die-hard partisan would be forced to agree.
There is no other reasonable conclusion once you know the critical features of Major NCD (dementia). To receive this diagnosis, you must show a “significant” (DSM-5 descriptor) decline from a previous level of performance in one of the six cognitive domains — attention, executive functioning, learning and memory, language, perceptual-motor skills, or social cognition. With dementia, there is usually a decline in all six areas. Those declines “interfere with independence in everyday activities.” This interference is generally measured with Activities of Daily Living (ADLs) scales that assess six primary areas of personal care: dressing, bathing, getting in and out of bed or chair, walking, using the toilet, and eating.
Major NCD (dementia) is a deteriorating condition. There is no cure for it. Individuals with dementia have little insight into their condition, a feature which spares them some emotional suffering. But it is a fateful diagnosis — for the patient and all those in his orbit.
Goldwater Rule Considerations
The gravity of diagnosing Mild or Major NCD brings with it ethical and scientific responsibilities. The effort by mental health professionals to diagnose or offer informed opinions about Biden’s or Trump’s possible neurological impairment reprises the question of whether it is ethical, or even possible, to provide such opinions when you have not personally examined such public figures and do not have their consent. That issue was hotly debated after Trump was elected in 2016, when a number of mental health professionals went on record about his possible dangerous mental health vulnerabilities (see here, and here for discussion of that issue).
While I believe that issue has been resolved in favor of communicating our informed opinions to the public, I now think it is timely to summarize and reiterate those arguments in the context of the current focus on the possibility that one or both of our presidential candidates might actually meet diagnostic criteria for the distinct and consequential condition of Neurocognitive Disorder as defined in DSM-5.
This brings us to the Goldwater Rule…
Section 7.3 of the code of ethics of the American Psychiatric Association, enacted in 1973, has been coined the Goldwater Rule. The rule states that, concerning public figures “it is unethical for a psychiatrist to offer a professional opinion unless he or she has conducted an examination and has been granted proper authorization for such a statement”. The other significant mental health organization, the American Psychological Association, endorsed the Goldwater Rule in 2016 when then-president Susan McDaniel asserted in an op-ed to the New York Times, “The American Psychological Association wholeheartedly agrees that neither psychiatrists nor psychologists should offer diagnoses of candidates or any other living public figure they have never examined.”
These ethical guidelines are called the Goldwater Rule because, during the 1964 Presidential campaign, FACT magazine (now defunct) invited psychiatrists to participate in a survey of the psychological makeup of candidate Senator Barry Goldwater. Psychiatrists who responded branded Goldwater with various diagnoses and descriptors, such as “paranoid”, “schizophrenic”, “psychotic”, and “narcissistic”. Most responders claimed Goldwater was “dangerous” and unfit to be president. Goldwater later successfully sued the magazine for libel. The verdict in that case, and the episode as a whole, damaged the reputation of mental health professionals. And deservedly so, since most conclusions were not based on a rigorous or objective assessment or tied to scientifically-based knowledge.
The discussion around the Goldwater Rule revolves around two questions: is it ethical to diagnose a public figure “from a distance”? That is, should we? And is it possible to validly diagnose “from a distance”? That is, can we? Our two major mental health associations, the two APA’s, continue to say “no” to both questions.
Thus, we have an obligation to address these questions in turn.
Should We Diagnose Neurocognitive Disorder at a Distance?
About whether it is ethical to diagnose public figures at a distance, supporters of the Goldwater Rule cite three concerns related to violating the rule: (1) potential harm to the reputation of the public figure, (2) compromising the confidentiality and consent principles of the profession, and (3) potential harm to the reputation of mental health professionals.
These are legitimate concerns. Calling Barry Goldwater’s mental health into question was stigmatizing and harmful to him. The Goldwater episode also stained the reputation of mental health professionals who were seen as making politically motivated, unsubstantiated claims about Goldwater’s mental health and fitness for office. The Goldwater Rule was an understandable response to an armchair diagnosis that lacked a scientific foundation. Indeed, one lesson of the Goldwater affair is to approach diagnoses of public figures with caution, humility, and rigor.
However, the concerns over giving professional opinions about public figures need to be weighed against two other cornerstone ethical principles from the Code of Ethics of The American Psychological Association: the “duty to warn”, and the “responsibility to participate in activities contributing to the improvement of the community and the betterment of public health”. The duty to warn guideline stemmed from a California Supreme Court decision in 1976 (the Tarasoff case), which placed a legal duty on mental health professionals to breach confidentiality and warn a public member who might be at risk of serious harm. The responsibility to engage with the “betterment of public health” encourages mental health professionals to educate the citizenry about hazards to the general welfare.
We have both a duty to warn about potential harm and an obligation to share such concerns with the broader community. Many of us believe that our good faith and scientifically grounded arguments about the ex-President’s dangerousness override the strictures of the Goldwater Rule.
There is another standard for communicating psychological findings to the public, coined by the term “duty to inform”. This principle is based on the idea that an informed citizenry is essential for a functioning democracy. Citizens have a right to any relevant and meaningful information for those in office or seeking office for positions of power that affect the general welfare. This should include information about their health and competency. For example, if a candidate were diagnosed with a medical condition and was not expected to survive their term in office, we would feel privileged to know that. If a candidate had a psychiatric condition that guaranteed he would inflict harm on others, we likewise have a right to know. And, if mental health professionals recognized that a candidate for high office displayed signs consistent with a progressive neurological disease that compromised their fitness for office, they would have a duty to share their concerns with the public.
The Duty to Warn and Duty To Inform principles make the case that we should appraise Donald Trump and Joe Biden from a distance and offer scientifically based opinions about their brain health. We now turn to the question of whether we can make substantive judgements about them without the benefit of a personal examination.
Can We Diagnose Neurocognitive Decline at a Distance?
The Goldwater Rule asserts that you need a face-to-face interview and examination to make any valid psychiatric diagnosis. However, over the past few decades, there have been numerous studies that refute the notion that a clinical interview is the “gold standard” of psychiatric diagnosis (see especially here and here).
These studies emphasize that there are three sources of data from which to form a diagnostic impression: from the patient, in the form of the clinical interview and examination; from informants, such as family, friends, work colleagues, journalists, and biographers; and from archival sources, such as taped interviews, real-time observations from news footage, social media output, and court records. It turns out the clinical interview is subject to all sorts of biases and distortions, including impression management on the part of the patient. What matters is the relevance and quality of the information that goes into making a diagnosis rather than where the information comes from.
There is abundant informant data on Biden and Trump in the form of biographies, magazine articles, insider accounts, and investigative reporting. And, of course, there is a wealth of archival data due mainly to social media and the televised nature of celebrity and the modern Presidency. This voluminous data is particularly significant in diagnosing Neurocognitive Disorder since it enables us to identify changes over time in critical diagnostic markers of this disorder, such as specific linguistic, reasoning, and memory difficulties. These deviations from an earlier baseline are essential to this diagnosis.
The core pillar of the Goldwater Rule — the necessity of a personal interview — has collapsed in the modern era under scientific scrutiny. Indeed, for certain types of diagnoses — Psychopathic Personality Disorder is one good example — a personal interview is not only not necessary but not even advised because of the patient’s skill in dissembling, which can confound the efforts of even expert clinicians.
We should offer professional impressions about public figures when we see a duty to warn or to contribute to an informed citizenry, and that we often can provide relevant opinions even without the benefit of a personal interview. Now, we need to consider the specific situation of Neurocognitive Disorder.
Given the nature of the assessment process for Neurocognitive Disorder, the answer to whether we can provide good-faith, authoritative opinions is less certain. Do we have sufficient and reliable data to diagnose Biden or Trump with Neurocognitive Disorder? As diagnosticians, we need to acknowledge that because Biden and Trump have not cooperated fully, we cannot engage in the ideal neurological assessment process. But it turns out, neither are we lacking meaningful data. Both points deserve elaboration.
What Are the Ideal Steps to Comprehensively Assess for Neurocognitive Disorder?
There seems to be a consensus among leading healthcare institutions (e.g., Mayo Clinic, National Institute Of Health) and advocacy organizations (e.g., Alzheimer’s Association, AARP) on the procedures prescribed to help arrive at a diagnosis of Neurocognitive Disorder. Experts emphasize five steps:
1. Secure a detailed medical history.
2. Perform a physical and neurological examination to test the patient’s senses and movements and a mental status interview to assess memory, attention, judgment, and insight.
3. Neuropsychological testing to carefully assess strengths and weaknesses across multiple areas, particularly in the six cognitive domains listed in DSM-5. Testing can provide a baseline, measure changes in functioning, and pinpoint spheres of cognitive dysfunction.
4. Brain imaging tests like MRI, CT, and PET scans. Such scans cannot diagnose dementia on their own, but they can help identify where damage might have occurred and the possible cause of the dementia.
5. Lab tests to check for conditions that might be contributing to cognitive decline. There is no stand-alone lab test for dementia. However, standard lab work can help rule out certain conditions implicated in dementia or provide biomarkers that might suggest a particular subtype.
Relevant Data from Biden’s and Trump’s Released Medical Reports
Regarding the diagnosis of NCD in Biden or Trump, in an ideal world, all the above steps would be taken, and the results would be shared with the public. In the real world, there is no legal requirement that the President or candidates release a health report. That legal reality, coupled with the exigencies of presidential politics, has resulted in the public having some, but not all, of the desired data that could be generated from the candidates if they fully participated in the five diagnostic steps noted above. From my Google search efforts to cull the medical information available and relevant to the diagnosis of NCD in Biden and Trump, I will summarize what we do have vis a vis the five diagnostic steps noted above.
For President Biden
1. As president, Biden undergoes an annual physical exam. His latest exam was in February 2024. His physician, Kevin O’Connor, released a six-page report this past February 28th (available to the public here). In that letter, Dr. O’Connor notes, “I have conducted a comprehensive review of President Biden’s medical history and performed a detailed physical examination.”
2. Specialists from several fields, such as cardiology, orthopedics, and others, reviewed Biden’s medical history and participated in the examination. Neurology was one of those specialty areas, as noted in the report: An extremely detailed neurologic exam was again reassuring in that there were no findings which would be consistent with any cerebellar or other central neurological disorder…
There is no report of a mental status exam. However, it should be noted that a mental status exam is not typically considered part of an annual physical (I have never had a mental status exam in any of my physicals).
3. He has not undergone any neuropsychological testing. During the daily press briefing on the day Biden’s health report was released, White House press secretary Karine Jean-Pierre said Biden’s physician assessed that the president “doesn’t need a cognitive test,” also noting Biden “passes a cognitive test every day” because he constantly “moves from one topic to another topic, understanding the granular level of these topics.”
4. I could find no report of any brain imaging testing.
5. President Biden, in his February 2024 physical, had extensive lab work, including a comprehensive metabolic panel, a complete blood count, urinalysis, and tests of thyroid functioning. There appear to be no significant abnormal lab results, which might result in concern over early dementia or the presence of any illness that leads to dementia.
Health Reports for Ex-President Trump
1. We have less information about Trump’s medical history or recent physical examinations. In 2015, his physician, Dr. Harold Bornstein, issued a statement declaring that Trump “will be the healthiest individual elected to the presidency,” along with several other superlatives about his physical condition. However, three years later, Bornstein admitted to CNN that Trump “dictated the whole letter. I didn’t write that letter.”
The most recent report on his health status came on November 20, 2023, in the form of a three-paragraph statement posted on Truth Social where his current physician, Bruce Aronwald, D.O., described Mr. Trump’s health as “excellent.” The report has been characterized as “fawning and vague.”
2. In that 2023 statement, there was no mention of a neurological exam, but there was an assertion that Trump’s “cognitive exams were exceptional.” However, no detail was provided about what “cognitive exams” were administered or Trump’s actual performance. Trump himself has not spoken of any recent “cognitive exams,” which is curious since he has never hesitated to boast about his physical and mental prowess.
From his 2018 physical, his doctor Ronny Jackson stated, “Neurological exam Examination of the cranial nerves, cerebellar function, deep tendon reflexes, motor function, and sensory system were all normal.”
3. Trump has engaged in neuropsychological testing, albeit only a smidgen. In 2018, Trump reported that he had taken the Montreal Cognitive Assessment Test (MoCA), a one page, 30-point test that can be administered in 10 minutes. The MoCA is considered an initial screening device that can detect signs of possible dementia. It should not be regarded as a comprehensive screening device like a mammogram or colonoscopy.
Trump reported that he got a perfect score of 30, claiming that doctors told him that “rarely can anybody do what you just did” and that the test contains “very hard” questions, particularly the last five. In fact, the average score on the test is 27 (and even that average is taken from a sample of people suspected of cognitive impairment). A score of 30 is considered normal, not exceptional.
It is hard to tell if Trump is serious or self-aggrandizing in his characterization of the MoCA as “hard.” Examples of questions near the end, the supposedly difficult part of the test, include repeating a sentence out loud, naming as many words as you can starting with the letter F, trying to identify the similarity between different objects such as trains and bicycles (modes of transportation), and saying what the current date is. Dr. Jonathan Reiner, professor of Medicine and Surgery at George Washington Hospital, wryly observed, “If you think a dementia screening test is very difficult, you may have early dementia.”
Still, we should note that Trump’s performance in the average range of the MoCA is a data point relevant to the diagnosis of Major Cognitive Disorder (dementia). However, it does not add much to what we observed and knew about Trump in 2018. To receive such a diagnosis would have required concrete deficits in independent living skills, such as attending to personal hygiene, ability to pay bills, or managing one’s medication. We know the president lives in a bubble and has a large staff to meet his needs. Still, it would have been impossible to hide significant struggles with independent living from the public. Trump’s performance on the MoCA only reinforced the obvious reality that Trump was not in the throes of full-scale dementia (Major Neurocognitive Disorder) when he was living in the White House.
(Trump has challenged Biden to a duel of cognitive testing. The MoCA would provide little information from what we already can observe. However, a full neuropsychological battery with many challenging tasks to assess multiple cognitive domains, typically taking 5–8 hours to administer, would be substantive and informative. However, of course, no one should take seriously the prospect of Biden or Trump submitting to such a test).
4. I could find no reports of brain imaging studies on Trump.
5. In his doctor’s November 2023 statement and his 2020 annual physical, Trump’s lab results were reported to be within normal limits. We should note that, in contrast to Biden’s recent health report, no specifics on lab work were provided.
A few other observations about the candidates from the health records available to the public:
1. Trump’s father, Fred, was diagnosed with “mild senile dementia” in 1991 at the age of 85. Three years later, the diagnosis was upgraded to Alzheimer’s. Individuals with a first-degree relative, such as a parent, who had Alzheimer’s, are more likely to develop the condition — their risk increases by about 30 percent. Scientists have identified the gene implicated in the transmission of Alzheimer’s. It is called apolipoprotein4 (APOE4). While identifying this gene may not fully predict whether an offspring will develop Alzheimer’s, a recent study suggests its presence may be a cause, not just a risk factor for Alzheimer’s. Testing for the gene is safe, straightforward, and inexpensive. I could not find anywhere in his reported health records that Trump had submitted to that genetic test.
2. Some have pointed to Biden’s stiffening gait over the years as a possible sign of early dementia. It is, therefore, noteworthy that his gait difficulties were directly addressed in his most recent physical exam. Based on a detailed neurologic exam and a review of radiologic imaging, his team of doctors concluded: “that much of his stiffness is, in fact, a result of degenerative (‘wear and tear’) osteoarthritic changes of his spine.”
Likewise, some neurological experts have pointed to Trump’s forward listing posture, jerky arm movements, and odd circular gait as possible signs of early dementia. None of these potential clinical signs have been directly addressed in any of Trump’s health reports.
3. When the results of his 2019 physical were released, Trump had tipped into the formal category of obesity. Obesity is a risk factor for brain atrophy and cognitive decline in general, as well as Alzheimer’s dementia in particular.
What can we conclude about the brain health of Biden and Trump from the medical reports available to the public?
First, the medical information Biden’s team of doctors provides is more comprehensive and detailed. Also, Biden’s health reports are more objective, whereas Trump’s doctors often politicize his health claims, as evidenced by hyperbolic claims such as “astonishingly excellent” and “his cognitive exams were excellent.” Thus, Biden’s camp’s assertions about his health status rest on firmer scientific ground.
Second, concerning the possibility of diagnosable Major Neurocognitive Disorder (dementia) or even Minor Neurocognitive Disorder (likely early dementia), if we only look at the evidence from the public records — for Biden and Trump — it is hard to assign such a diagnosis. Neither man is reported to suffer from diseases associated with dementia, such as Alzheimer’s, Parkinson’s, Pick’s Disease (also known as frontotemporal dementia), or impaired blood flow to the brain (vascular dementia). Nor are there other clinical findings cited from their public reports that would warrant a formal diagnosis of dementia.
However, it should be emphasized, nor is there sufficient data from the official reports to rule out the possibility of Mild Neurocognitive Disorder. The information generated by the annual physical is simply not sufficient to meet the demands of a state-of-the-art comprehensive neurological examination. We need more pertinent data. Fortunately, we are not bereft of such data.
What Can Archival Sources Tell Us About Biden or Trump’s Brain Health? Let’s Go to the Videotape
There is a treasure trove of pertinent data to be mined by direct observation of Biden and Trump through archival sources. Videotapes of Biden and Trump over the years have afforded an abundance of behavioral observation data that can be culled for behavioral markers relevant to Neurocognitive Disorder. As a profession, neurology relies on direct observation more than any other clinical skill. As noted earlier, it is not the source of information that is crucial in diagnosis but its quantity, quality, and relevance.
For Trump it is hard to imagine another individual for whom there is so much videotape material to analyze. Trump is arguably the most chronicled celebrity/President/ person in history. His spotlight has generated a wealth of archival information, which is good news for those seeking meaningful diagnostic markers of the six cognitive domains listed in DSM-5. While there may be less such material on Biden, there is plenty enough to evaluate the presence or absence of those markers.
Access to so many behavioral observations over many years brings with it several benefits. First, we can observe whether there have been changes over time in critical areas of functioning. Remember, the diagnosis of Neurocognitive Disorder revolves around identifying certain kinds of (non-aging) declines from an earlier baseline level of functioning. For example, assessing speech samples over many years enables us to measure possible decline in the language domain.
Second, the volume of data available through archival sources can enhance the validity of our findings. Observing Biden and Trump’s behavior, often in many different situations, provides non-overlapping data that can contribute to incremental validity. Such data can provide evidence of persistency (a diagnostic trait displayed consistently over time) or a change in baseline (diagnostic trait changes over time). We also get a good measure of pervasiveness (diagnostic trait displayed across situations). Voluminous data across many contexts also allows the diagnostician to take advantage of statistical aggregation, which minimizes random error by canceling out outlier displays of behavior that can be misleading.
Third, we can use the archival data to zero in on each of the six vital cognitive domains stipulated in DSM-5 used in the NCD diagnosis. Keep in mind we only need to demonstrate a decline in one domain to consider a diagnosis of Neurocognitive Disorder. We nevertheless will appraise Biden and Trump in all six domains.
Evaluation of the Language Domain
We will start with the language domain since it offers a rich data source to help identify possible neurological dysfunction. Compared to the other five domains, language samples are voluminous, allow for direct observation by the diagnostician, and are relatively easy to rate. The other five domains are trickier to evaluate because those behaviors occur primarily off-camera, limiting the sample size of behaviors you want to analyze.

Also, a comprehensive review of studies on the use of language measures to identify Mild and Major NCD concluded: “Based on our research, we are inclined to claim that (NCDs) can be more sensitively detected with the help of a linguistic analysis than with other cognitive examinations.” Further confirmation that certain kinds of verbal behavior indicate slippage in brain function can be found here.
What are some of the fine-grain verbal expressive markers linked with NCD? John Gartner has pointed out some key markers in recent interviews and articles. Piggybacking on his observations and using markers validated in the studies noted above, the following table presents seven verbal expressive markers linked to probable brain disease and not to normal aging.
Table 1: Verbal Markers Linked To Neurocognitive Disorder
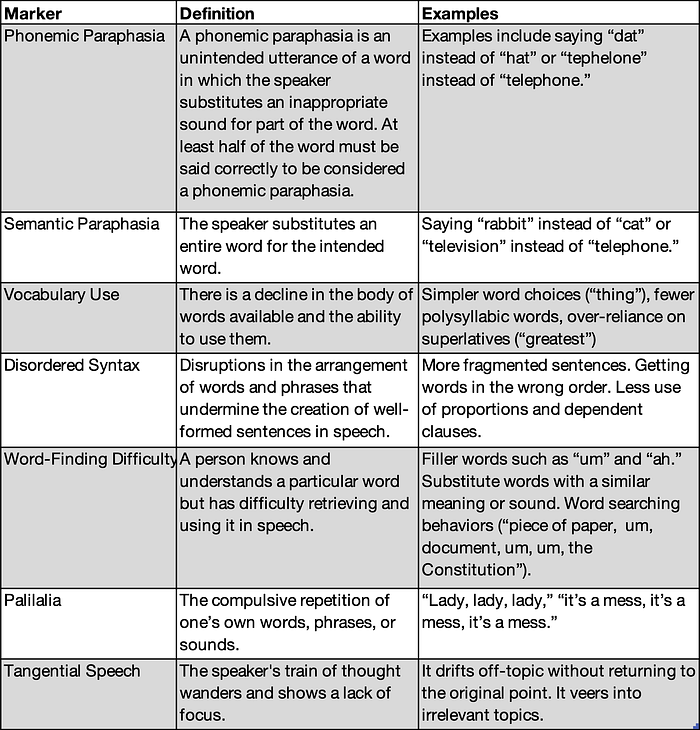
Because of their specificity, these markers allow for a more objective determination of cognitive decline in the language domain. Because of their empirical support, they allow for a more valid determination of clinically meaningful decline.
The next diagnostic step is to work out how to apply these markers to Biden’s and Trump’s speech. Much of the recent conversation about possible dementia has been accompanied by video mashups of Biden or Trump’s verbal struggles. Of course, these video mashups are produced by partisan actors and are not really aimed at sparking a scientific inquiry. Here is a typical mashup of Biden and one of Trump. Still, armed with our set of clinical markers, we can bring scientific scrutiny to these mashups and achieve some insight. Or perhaps not.
Why Video Mashups Are Not a Good Source for Evaluating Cognitive Decline
Video mashups can lead to false impressions and erroneous conclusions because of two fundamental methodological flaws. First, these mashups cherry-pick someone’s worst moments from a vast sample of behavior. We see many glitches but don’t get an accurate sense of how frequently they occur. If we saw a mashup of Steph Curry’s 20 worst moments during an NBA season, you’d wonder why he hasn’t been drummed out of the league.
These mashups run the risk of what is referred to as a “base rate fallacy”, where one focuses on an instance of a particular kind of problematic behavior and downplays or ignores the rate of relevant non-problematic behavior. In mathematical terms, one only pays attention to the numerator while ignoring the denominator. A good example comes from some of Biden’s video mashups, which show him stumbling slightly as he boards Air Force One (this same clip is used in several of the mashups). The clip is usually accompanied by ominous music and commentary such as “The man is falling apart in real-time.” Really? If an athletic twenty-year-old’s every movement outside the home was filmed over a month (much less years), don’t you think you would find similar moments?
The second methodological flaw revolves around the fact that any glitch is fodder for the video mashup. There is no effort to distinguish between which glitches are relevant to the diagnosis of dementia and which ones should be ignored. All glitches are treated as equals, which they are decidedly not. When they are strung together in a two-minute videotape, the impression created is one of clearcut senility.
These mashups leave us susceptible to the “what you see is all there is” bias, popularized by Nobel Prize-winning psychologist Daniel Kahnemann in his book Thinking, Fast and Slow. This bias refers to our wired-in tendency to believe that the information we have right in front of us is all the relevant information there is.
The markers from Table 1 could serve as a countermeasure to this kind of bias. Video mashups provide examples of behavior that might prove clinically meaningful if filtered through empirically validated markers. The problem, of course, is few viewers know about such markers or will go to that trouble.
In addition to not putting too much weight on video mashups, there is another methodological implication to understanding the “what you see is all there is” bias. Because of their age, Biden and Trump can display speech and language behavior that can look and sound like indicators of a neurological disorder but are just signs of normal aging. When we see an older person stumble or lose track of a conversation or, at times, have trouble finding the right word, it is easy to worry there might be something seriously wrong with the person. However, if these behaviors are not pervasive, we should not be concerned about a severe compromise in cognitive functioning.
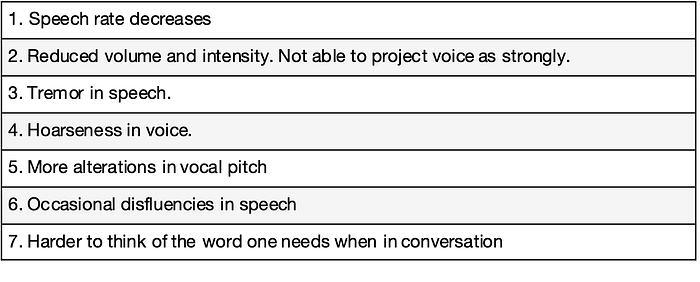
As diagnosticians and voters trying to judge one’s fitness for office, we want to do anything we can to separate the wheat of brain illness and meaningful cognitive decline from the chaff of normal aging and cognitive soundness. Table 2 provides a checklist of verbal markers of normal aging, most concerning vocal quality. It would be useful to apply this list, along with the list of markers from Table 1 to Biden and Trump’s recent speech behavior to distinguish signs of normal aging from signs of probable cognitive decline.
Table 2: Verbal Markers of Normal Aging
In a similar vein, we need to consider President Biden’s diagnosed stuttering condition, which can often be misconstrued as a sign of cognitive impairment. Stuttering, also termed Childhood-Onset Fluency Disorder in DSM-5, is a disturbance in the usual fluency of speech. While stuttering is a problem, it is not associated with any cognitive or psychiatric impairments. Indeed, for reasons that are not clear, the IQ of the average stutterer is 14 points higher than the national average.
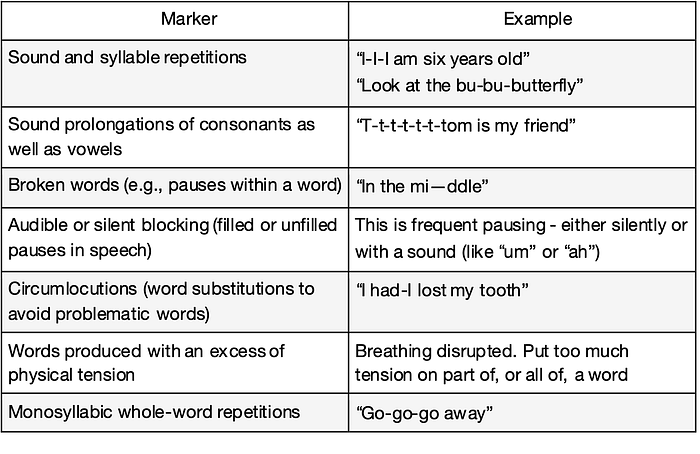
However, the symptoms of stuttering can be disconcerting to observers and lead to a misimpression about possible cognitive impairment. A checklist of stuttering features (Table 3) can help diagnosticians (and observers) pinpoint instances of stuttering to help ensure they are not counted as signs of possible deteriorating brain disease, which they are certainly not.
Table 3: Verbal Markers of Stuttering
When all three checklists are used together to evaluate the language domain, they enable raters to distinguish signs of cognitive decline from the features of normal aging and stuttering (differentiating phonemic paraphasia from the occasional disfluencies of normal aging and from the sound and syllable repetitions of stuttering, is but one example).
Armed with the checklists, we can now analyze more objectively the possibility of a meaningful decline in the language domain. How do we go about this analysis? There could be several ways, but here is the path I took:
1. Select videotape cuts randomly from the present and the past where Biden and Trump are speaking. It is best to get a range of speech samples, such as formal speeches, press conferences, one-on-one interviews, and, most importantly, unscripted utterances. Fortunately, there is no shortage of such videos on YouTube.
2. Catalogue each instance of the seven verbal markers linked to possible dementia listed in Table 1. Use the other two checklists for each example to consider whether the instance might be a sign of normal aging or stuttering instead.
3. Then, make two comparisons. First, the number of markers for each candidate should be compared separately over time (samples from the 1980s and 1990s were compared to samples in the past year for Biden and Trump) to determine if there has been a shift in these key markers for either candidate. Second, compare the number of markers between Biden and Trump from their more recent verbal utterances.
4. To categorize the frequency of markers for each candidate in the past and present, I used what is referred to as a 5-point Likert scale as follows:
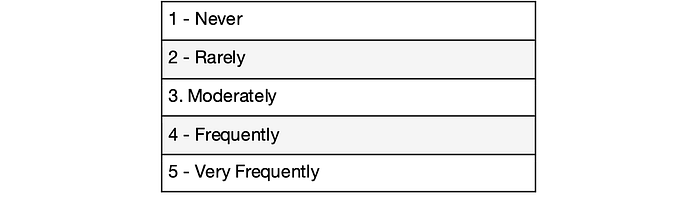
This suggested methodology helps eliminate cherry-picking by randomly choosing speech samples from an ample supply. It also reduces “what you see is all there is” bias by relying on evidence-derived checklists to guide your observations and a frequency rating scale to measure those observations more objectively.
Differences Between Trump and Biden on Verbal Markers Linked to Possible Dementia
Phonemic paraphasia
Phonemic paraphasia is the substitution of non-words for words that sound similar. The nonword preserves at least half of the intended word’s syllables. Trump has displayed this marker frequently over the past few years. Gartner has cited several of his slip-ups. For example, beneficiaries became “benefishes, “Obama became “obamna,” midterm elections became “midtowm,” Christmas became “Chrissus,” and Venezuela became “Venezwheregull.”
Here is a brief clip of Trump exhibiting phonemic paraphasia.
Biden also has disfluencies in his speech, some of which could be mistaken for phonemic paraphasia by an untrained observer. However, knowing the difference between stuttering and paraphasia can eliminate such mistakes. Phonemic paraphasia is an unintended utterance, while stuttering is a struggle over an intended utterance. Also, phonemic paraphasias come out relaxed from the speaker, whereas there is often noticeable anxiety with the stutterer. Biden’s disfluencies are consistent with his stuttering condition when he anxiously, but unsuccessfully, tries to produce a letter or word he has in mind.
Semantic paraphasia
Semantic paraphasia occurs when an entire inappropriate word is substituted for the intended word — for example, calling a lamb a dog.
Biden did display these errors, although only very occasionally, and, interestingly, in the past and present. Trump exhibited semantic paraphasias much more frequently — not in every speech sample but in a moderate percentage. As a middle-aged man, he did not seem to have this difficulty. His speech then might be characterized as glib but not marked by the use of totally incorrect works.
Here is an excellent example of semantic paraphasia: a video of Trump repeatedly using the word “oranges” when he obviously meant to say “origins.” Again, see Gartner for a more comprehensive listing of Trump’s recent incidents of semantic paraphasia.
Vocabulary
The vocabulary marker is defined as a drop-off in the body of words available to a speaker and the ability to use them appropriately. Vocabulary skill seems to be a particularly valid sign of possible early dementia because it is not a capacity that declines with normal aging. If anything, there appears to be a slight increase in vocabulary as one gets into one’s seventies and eighties.
What do we observe in Biden’s and Trump’s vocabulary usage over the years? First, it is fair to note that neither Biden nor Trump are considered to be one of our more intellectual presidents. Their unscripted speech has never been peppered with SAT words. However, their vocabulary skills as middle-aged men, perhaps unremarkable, are solid, even above average. For example, in one interview, Trump used words such as “verve,” “aesthetically,” and “innocuous.”
That is why the shift in Trump’s vocabulary is striking. To appreciate the change, I suggest you look at interviews with Trump in the 1980s and 1990s. You can do your own Google search, but these interviews with Barbara Walters, David Letterman, and the BBC are representative. If we kept his identity hidden and compared the transcripts of Trump’s speech then and now, you wouldn’t believe they were the same person.
Biden has yet to show any noticeable decline in vocabulary over the years. If you compare Biden’s transcripts as a middle-aged man to recent interviews, he would sound like the same guy. His words may come out more slowly, but you don’t see the drop-off in the range or appropriateness of his vocabulary. In contrast, with Trump, you see a shift to more superlatives and monosyllabic words in his speech.
For this marker of vocabulary use, we also benefit from two studies that have examined Trump’s verbal behavior, with a particular emphasis on vocabulary. Trump Wasn’t Always So Linguistically Challenged. What Could Explain The Change? Sharon Begley wrote the article under the auspices of STAT, a media and journalism company that distills information about health and medicine. STAT took decades of on-air interviews with Trump to compare with interviews after he was inaugurated in 2017. They took this material to experts in neurolinguistics, cognitive assessment, and clinical psychiatry for their informed opinion: “They all agreed there had been a deterioration, and some said it could reflect changes in the health of Trump’s brain.” In their appraisal, the experts emphasized the shift from a sophisticated vocabulary to a simpler one, along with his difficulty stringing sentences together. They noted the changes were “striking and unmistakable.”
In Trump Speaks at Level of 8-Year-Old, New Analysis Finds, Emily Shugerman reported on the findings by factba.se, which studied the “off-script” remarks of all the presidents from Trump back to FDR. They subjected those remarks to eight different tests for vocabulary complexity, diversity, and comprehension level. They found “On every single test, Mr. Trump scored the lowest.” Compared to the other presidents, Trump used significantly fewer syllables per word and significantly fewer unique words. The sample of Trump’s speech analyzed was from his first year in office, at which point his vocabulary skill level appears to have diminished from his middle-age years.
Word-finding difficulty
We all experience this when we have a word on the tip of our tongue but can’t retrieve it. In that moment, we often resort to filler words such as “um” or “ah” as we search for the word. If we can’t find the word, we often produce a non-specific noun such as “thing” or “person”. This word-finding difficulty gets worse as we age. However, if pronounced, it may be a sign of Neurocognitive Disorder.
In an interesting study relevant to this subdomain, cognitive neuroscientists analyzed the speech of President Reagan and the first President Bush from their press conferences. They found President Reagan displayed significantly more filler words and indefinite nouns than President Bush. Reagan, in a letter to the public five years after leaving office, acknowledged that he had been diagnosed with Alzheimer’s disease. By all accounts, Bush appeared to have good cognitive health until he died at age 94.
The same methodology from that study was applied to then-President Trump’s speech in 2018 and reported by The National Institute of Health in An Empirical Analysis of Popular Press Claims Regarding Linguistic Change in President Donald J. Trump. The investigators found that there was a “systematic increase in use of filler words “for Trump that is not significantly different from that previously observed for President Reagan” and is significantly greater than that found in President Bush’s speech.
Although not a subject in that study, Biden occasionally uses filler words and non-specific nouns in his speech samples. However, the rate of these difficulties does not appear to have increased as he has aged.
Palilalia
Palilalia is the involuntary repetition of a word or phrase. It often occurs at the end of a spoken sentence, and the individual’s speech usually decreases in audibility with each repetition.
Involuntary is the crucial word, especially when it comes to Trump, who is known for repeating phrases as a rhetorical strategy to engender what psychologists term the illusory truth effect, which refers to the phenomenon that when we are repeatedly exposed to misinformation, we are more likely to believe it is true. Want to make a lie seem true? Unfortunately, the answer appears to be repeat it again and again, taking care to use the same phrase. Critics of Trump contend this is one of the reasons he persists in his well-documented pattern of lying: it works. On any account, this kind of repetition is not an indicator of cognitive decline. Indeed, many view it as high-level cunning.
However, this repetition by Trump certainly seems involuntary. I could find no such incidents when Trump was younger. He does not display this neurological glitch frequently today, but it is clinically significant behavior.
I could find no incidents of Biden displaying this repetition of words or phrases, which might seem surprising given his stuttering problem. He occasionally displayed repetitions of letters and syllables — consistent with his stuttering diagnosis — but not at a greater rate than when he was younger.
Disordered syntax and tangential thinking
Disordered syntax is characterized by speech that contains a large number of incomplete sentence fragments. The speaker struggles to communicate in complete sentences in unscripted speech. Tangential speech is when the speaker wanders off and struggles to maintain focus. Disordered syntax is the breakdown of coherence within a particular sentence, whereas tangential thinking is the inability to string sentences together without a mid-thought subject change. We all display these communication mishaps occasionally. However, if they become prominent in one’s speech, they suggest Neurocognitive Disorder.
We lump these two subdomains together because they often occur together and can be challenging to tease apart. Take this recent example from Trump:
“Over the seas and over our land. And then they want us to have clean. I said wait, we’re gonna be clean but it’s all flying. Just remember that. Does that make sense? In other words, it’s all coming through the currents through the air, they can name it”
Does this excerpt represent a problem speaking in complete sentences (“me Tarzan/you Jane” mode), or an example of his thoughts wandering, or both? These head-scratching examples of fragmented speech and thought are becoming all too familiar for Trump. They can be found in most of his recent unscripted speech samples and earn the rating “very frequently” on our Likert scale. The tortured syntax and tangential speech can rarely be found in the archival tape on Trump from the 1980s or 1990s, underscoring the significant shift in these language behaviors.
In the past and present, Biden occasionally has trouble completing his thoughts. But the quality of his difficulties is different. Instead of producing word or sentence fragments, he sometimes displays great effort in getting a word or complete thought out. He then might use an indefinite word like “anyway” or “whomever” or just not complete his thought, with his voice trailing off. Commentators have described these moments as signs of Biden’s “confusion.” A better descriptor would be “struggle.” He seems acutely aware that he is not communicating ideally, sometimes even commenting on his struggle with a phrase such as “let me say another way,” or “might not be able to pronounce…”. This is classic stuttering behavior.
Trump’s voice never trails off. His voice usually remains strong and unwavering even amid a particularly discombobulated utterance. Trump seems oblivious to these moments of verbal confusion, like a running back barreling into the secondary who doesn’t realize he fumbled the ball shortly after getting the handoff.
Summary of the Findings in the Language Domain
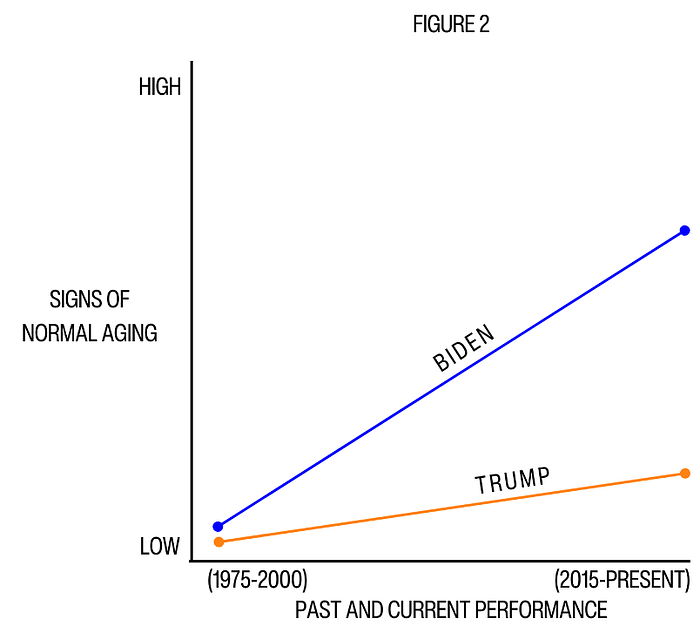
The differences between the two candidates in the language domain were compelling and prognosticative. President Biden did not display any meaningful decline with any of the markers of Neurocognitive disorder. He “never” or “rarely” displayed any signs of those verbal struggles thirty years ago, and he “never” or “rarely” shows those signs today. Ex-President Trump displayed shifts in all seven markers, receiving rankings of “never” or “rarely” in the past versus “moderately” or “frequently” today. There are also independent studies attesting to his vocabulary drop-off and word-finding difficulty.
Trump shows signs of cognitive decline beyond normal aging. Biden does not.
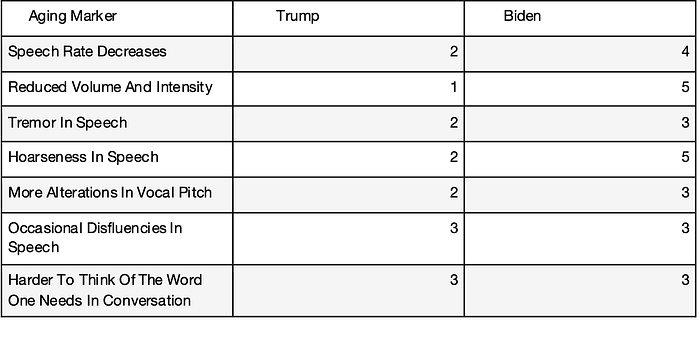
It probably should also be noted that I placed Biden in the “frequently” category for signs of normal aging in this verbal domain. In contrast, I thought Trump deserved to be in the “rarely” or “moderately” category for indicators of normal aging. That difference has mostly to do with voice quality. Biden’s voice is noticeably weaker and more hesitant. Biden has also recently developed a tendency to cough and clear his throat more often, which undoubtedly adds to his perception of his frailty. In his recent physical report, this was explained as a symptom of his gastroesophageal reflux.
These findings are summarized in the tables and figures below.
Table 1: Frequency of Past Behaviors (1975–2000) Linked to Neurocognitive Disorder
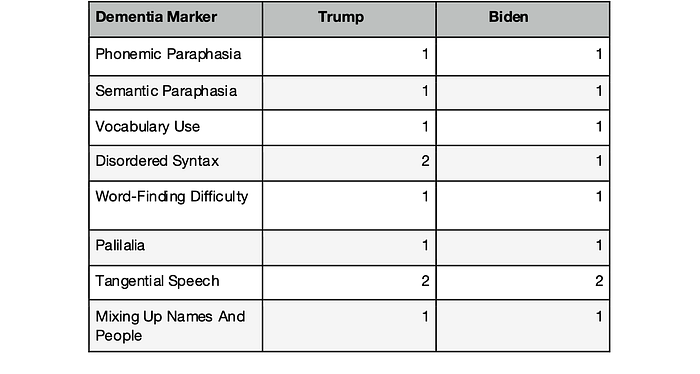
Table 2: Frequency of Verbal Markers Linked to Neurocognitive Disorders (2015 — present)
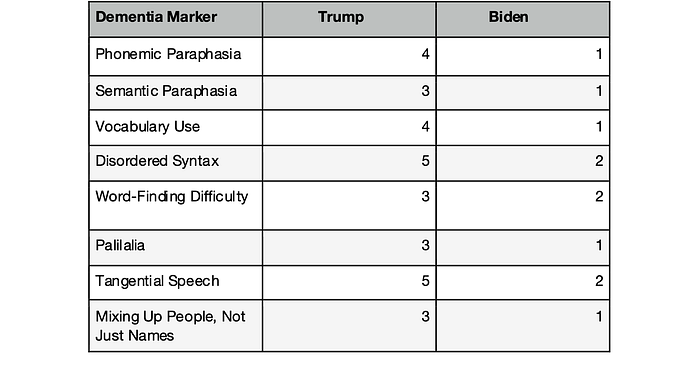

Table 3: Frequency of Signs of Normal Aging
Diagnostic Considerations of the Findings in the Language Domain
Based on the findings, does Trump warrant a diagnosis of Mild Neurocognitive Disorder? (Biden is not under consideration since he did not display declines in the key language markers). Two basic criteria must be met:
1. Evidence of modest decline from a previous level of performance in one or more of the six cognitive domains; and,
2. the cognitive deficits do not interfere with the capacity for independence in everyday activities but require greater effort, which may manifest in compensatory strategies such as more list-making.
The first criterion, as set out in DSM-5, sets a high bar by asking for evidence of cognitive decline that is “preferably documented by standardized neuropsychological testing or, in its absence, another quantified clinical assessment.” Unfortunately, but not surprisingly, we do not have any documented neuropsychological testing for Biden or Trump from the distant past. Nor do we have any recent neuropsychological testing for either candidate for the detection of early dementia (the Montreal Cognitive Assessment is a crude screening device to signal the possibility of advanced dementia, e.g., “see if you can point to the lion,” in a picture of a lion, a camel, and a rhinoceros).
Thanks to Biden’s and Trump’s statures and celebrity, what we have in the language domain is an enormous sample of observable behavior from which we can measure specific verbal markers of possible neurodegenerative disease. The abundant videotape allows for random sampling, which boosts objectivity. In addition, by using empirically derived checklists with operational definitions, we have conformed to the DSM-5 guideline of “quantified assessment”. Most importantly, the checklists enable us to compare each candidates’ language performance over time to see if there is meaningful decline; and to compare the difference between Biden and Trump on signs of early dementia at the present time.
The second DSM-5 criteria for Mild NCD — the emergence of some effort to sustain independent living — deliberately sets a low bar when it states, “greater effort, compensatory strategies, or accommodation may be required” (my italics for emphasis). There is no strict or operational definition of what that effort entails. “Effort” is mostly a subjective state that is often kept private and only detectable by those close to the patient. It is hard to prove if the patient himself or a loved one doesn’t acknowledge such an effort. Trump, aka the “very stable genius,” only brags about his superior mental state.
Effort may be evidenced in accommodations such as writing yourself reminders, using pill boxes, and keeping your space clutter-free. In that vein, many have noted that Trump now relies more heavily on a teleprompter at campaign events than he did as president. That is only one data point, but it is worth noting.
With these criteria in mind, Trump clears the bar of displaying modest or moderate decline in the language domain, thus meeting the first criteria for diagnosis of Mild Neurocognitive Disorder (early dementia). He also exhibits signs of struggle in his verbal utterances, his more significant reliance on a teleprompter, and his recent pattern of confusing people, not just names and dates.
Thus, ex-President Trump should be strongly considered for the diagnosis of Mild Neurocognitive Disorder.
Significance of the Findings
These findings are noteworthy with regard to the fundamental question of this article, namely, do Biden or Trump meet DSM-5 diagnostic criteria for a Neurocognitive Disorder and thus likely to be in the throes of an irreversible brain disease? To appreciate the gravity of being considered for such a diagnosis, let’s revisit what it means to go through that diagnostic porthole. There are three consequential implications.
First, if one receives the diagnosis of Mild Neurocognitive Disorder, there is a lot we can say about them, and we can say it with authority. That is because the significant revisions in classifying Neurocognitive Disorders in DSM-5 — identifying just three distinct syndromes with their cardinal features and prognostic course — were significant advances in providing a solid empirical foundation for the disorders. This clarity thus enabled clinicians and researchers to communicate more effectively, generating substantial advances in our understanding of NCDs since the publication of DSM-5 in 2015 (updated in 2022). Regarding Mild Neurocognitive Disorder, we have learned a lot more about its essential features, how to differentiate it from other conditions, its response to treatment, and, most importantly, its course and prognosis.
Second, with the Mild NCD diagnosis, we can now make assertions about the individual’s current functioning. Even though it may not be evident to the casual observer, the diagnosed individual has crossed a threshold into suboptimal functioning. Cognitive decline has set in, and it is beginning to have its way. The individual can still function independently, but there is now some struggle to sustain that independence. Also, while you need to demonstrate only a decline in one of the six cognitive domains for the diagnosis, there is likely some decline in most domains, even if it is subtle.
Third, we can make predictions about the individual’s future capacity. As noted earlier, the annual conversion rate for someone with Mild NCD to progress to Major NCD, where the capacity for independent living is lost, is around 15%. While some people with Mild NCD recover, it is because they have a condition — traumatic brain injury, alcohol abuse, and clinical depression are frequent examples — that is either acute or amenable to treatment. However, the majority of people with Mild NCD have a deteriorating brain disease that is destined to get worse and for which there is no effective treatment. You are particularly likely to be in this poor prognosis group if you receive the diagnosis after the age of seventy and have a family history of Alzheimer’s, two risk factors that Trump exhibits.
We will discuss the remaining five cognitive domains with an eye to Biden’s possible neurological decline and to see if there is more evidence of Trump’s decline. But I don’t want to bury the lead on the seriousness of these findings in the language domain. On March 2, 2024, John Gartner, Ph.D, founder of Duty To Warn, put out a petition to mental health professionals outlining the case for Trump’s neurological dysfunction. To date, over 2,000 have signed the petition. These findings of Trump’s decline in the language domain suggest they are standing on firm evidentiary ground.
Evaluation of Other Domains: The Memory and Perceptual-Motor Domains
The frustration over not having comprehensive neuropsychological testing for the candidates is well-founded with the domain of memory. Memory is complex. It has different processes (encoding, storage, retaining, and retrieval), different types (immediate, short-term, and long-term; sensory, visual, and procedural), and different ways of being measured (recall, recognition, and re-learning). There are fine grained tests of memory that, in principle, could pinpoint difficulties linked to meaningful cognitive decline. Since we don’t have data on memory performance from testing, we are left with archival (videotape) and informant (insider accounts) data to evaluate Trump and Biden’s possible memory struggles.

Both Biden and Trump display memory slip-ups in public that often are characterized as signs of serious decline. Biden’s errors typically involve mixing up names or words. Those mistakes are not evidence of neurological difficulty, although they often increase as one ages. Trump’s glitches are more concerning since they can involve confusing people. His recent rifts confusing Nikki Haley for Nancy Pelosi and Obama for Biden are good examples. If this type of confusion also occurs frequently behind the scenes, it would be a significant concern.
It is hard to make conclusive statements about serious memory issues from videotape. In contrast to language problems, memory issues can be more subtle and only be judged after extended observation. Is the individual consistently forgetting names? Or misplacing items (such as documents or makeup) around the house? Or forgetting appointments or important dates?
However, we can turn to informant data, as manifested in the many insider accounts of people who have worked closely with or observed the candidates up close, for additional relevant information. These insider accounts can be biased if the author is a partisan or a strong critic. Still, although he is criticized for his communication skills, Biden gets consistent praise for his off-screen executive functioning, including his sharp memory. He is described as focused, detail-oriented, and efficient in meetings.
Insider accounts of Trump often paint a picture of fecklessness and chaos in private meetings. One anecdote relevant to Trump’s memory function deserves to be highlighted. Michael Wolff, an author with significant insider access to Trump and his closest associates while he was president, reported that Trump had trouble recognizing a succession of old friends at Mar-A-Lago. That kind of difficulty is in the column of cognitive decline, not normal aging.
In summary, Biden is not displaying memory difficulties that would suggest meaningful cognitive decline. There is concern but insufficient data on Trump to rule in or rule out a moderate decline in memory function.
Perceptual-motor functioning, another one of the six domains in assessing Neurocognitive Disorder, involves our ability to coordinate our bodies’ movements to what is happening around us. That coordination requires the integration of motor (physical) and cognitive brain function. It covers many activities, including riding a bike and other sports, performing household maintenance and repair tasks, dancing, driving, and typing on a keyboard. Also, gait can be compromised by underlying neurological dysfunction.
As we age, we can struggle with activities we once took for granted. This can be just the vicissitudes of normal aging: we are not as strong, fast, or as coordinated as we were when we were younger. It could also reflect an orthopedic condition, vision difficulty, or other medical problem. Or it could be a sign of Neurocognitive Disorder. Unfortunately, just as we noted in the memory domain, we cannot avail ourselves of reliable and relevant neuropsychological testing results that could pinpoint perceptual-motor deficits that might be linked to neurological dysfunction. However, some findings from recently released medical reports are applicable to this domain.
Some have seized upon Biden’s cautious gait and occasional stumbles as evidence of dementia. Therefore, it is noteworthy that the issue of his gait was addressed in his latest physical, whose results were released on February 28, 2024. While noting that Biden’s gait stiffened noticeably after he incurred a hairline fracture while playing with his dog in 2020, the report said that the stiff gait is sustained by “degenerative (‘wear and tear’) osteoarthritic changes.” Also, the report asserts “a detailed neurologic exam” ruled out “neurological disorder” as a cause, although it did “support a finding of peripheral neuropathy in both feet.” These difficulties have not prevented Biden from working out five days a week and bicycling regularly.
As noted earlier, Trump released a three-paragraph letter from his doctor in November 2023. The report did not offer any details. Nor did it address any concerns about his gait or occasional odd physical movements.
However, two experts in clinical neurology have expressed concerns about Trump’s motor behavior based on their observations of him on tape. Richard Cytowic, textbook author and professor of neurology at George Washington University, cites the following abnormal behaviors in Trump as red flags of possible brain disease: his bent, forward-listing posture, his jerking right arm and right leg, slurred speech, and arm weakness. He urges the ex-president to get a brain scan so the public can be informed about his neurological health. Elisabeth Zoffmann, a forensic psychiatrist and associate professor at the University of British Columbia, also zeroes in on changes in Trump’s movement and gait over the years, “His walk appears wide-based and he has developed a swing of his right leg. He appears glued to the floor when he “dances” for his audience. If caught on camera standing still, he appears unnaturally immobile.” She speculates that he may suffer from Behavioral Variant Fronto-Temporal Dementia, an illness marked by deteriorating brain function and early death.
In summary, Biden does not display any memory or perceptual-motor difficulties that suggest cognitive decline beyond that associated with normal aging. Trump displays problems that indicate a possible decline. However, it is difficult to make conclusive statements about either candidate without more fine-grained neuropsychological testing in these two domains.
Evaluation of Biden and Trump in the Complex Attention, Executive Functioning, and Social Cognition Domains
Let’s begin by defining these remaining three domains of cognitive function used in DSM-5. Moderate or significant declines in any of these domains are linked to neurodegenerative disease.
Complex Attention — refers to our ability to focus on multiple things simultaneously. Can we choose what to pay attention to and what to ignore? Can we direct our attention to execute multiple steps to accomplish a goal?
Executive Functioning — refers to the high-level cognitive ability to control and coordinate other cognitive skills such as planning, decision-making, and organizing sets of tasks. It also refers to the process of regulating behavior, persevering, inhibiting undesirable behavior and responding to feedback.
Social Cognition — refers to the realm of emotional intelligence. It includes the ability to manage one’s own emotions and understand the emotions of others. It reflects the skills of self-awareness, the ability to defuse conflict, and the ability to connect well with others.

These three domains are lumped together because they pose a similar challenge to measure. While there is a wide range of neuropsychological tests to measure each of these domains, we do not benefit from such testing for Biden or Trump. Even if we could persuade them to take such a battery of tests, we would not have a baseline of similar test results from years ago to compare possible decline. Also, because these domains consist of a broad swath of behavior, much of it occurring off-camera, we cannot simply go to the videotape to look for specific markers that reveal possible decline.
To measure these domains, it would be helpful to pose questions like: What is he really like with family and friends? Is he a good ‘people person’ off camera? Is he able to run successful meetings? Is he a good problem-solver? Is he generally focused and persistent? Is he someone people enjoy working with? To get a decent appraisal, one must assess these behaviors over many situations and a good deal of time.
While information from videotape and other archival sources is not germane to these domains, information from close observers (colleagues, employees, family, friends, journalists who have had close access) or biographers with multiple insider sources could be relevant in assessing these more trait-like domains.
Fortunately, we are awash with such information, particularly for Donald Trump. He is arguably the most well-chronicled candidate in history. A partial list of informational sources would include 13 autobiographical efforts, 71 biographies, many of which are richly sourced, and hundreds of articles offering portrayals of the ex-president. There is less of this informant material on Biden, but plenty enough to provide many data points for these trait-like domains.
How do you distill all this information to gauge their performance in these domains? Using definitions of each domain, I cataloged scenes from books and articles where Biden or Trump was called upon to display complex attention, executive functioning, or social cognition. I favored scenes in which the cognitive domain was expressed on overt behavior (e.g., running a meeting at the White House), and the scene is well-resourced.
For each candidate, I then compared scenes from the present (past six years) to the past (before 2000) to evaluate possible decline. To bring a measure of objectivity to the exercise, I used a three-point rating scale of competency to grade their performance in the domains (1= weak, 2 = average, 3 = strong).
While I followed through with this good-faith social science playbook to cull the autobiographical material, I soon realized it wasn’t necessary to parse it so carefully and exhaustively. That’s because there was a strong consensus on how each candidate graded in these domains. There was not a lot of subtlety.
What do these biographies and insider accounts reveal?
For President Biden
Biden receives high marks in all three domains. While some drop-off in attention capabilities is a feature of normal aging, there do not appear to be any concerns from insider accounts about his focus. He is detail-oriented and apparently spends many nights after dinner reading scores of pages of briefing material to prepare for the next day’s agenda. He is known for his ability to synthesize a good deal of information and reportedly runs meetings in an organized and efficient manner. His reputation for reaching across the aisle and collaborating successfully with others also reflects well on his executive functioning.
Biden’s emotional intelligence is often lauded. He is known for his empathy. He appears to have close relationships and connects well with people, even if they may have different political orientations.
Of course, not all the material on Biden is hagiographic. He is also described as overly demanding of staff, too conciliatory, and having a quick temper.
There are a few well-sourced biographies on Biden. However, if you want a flavor of how he performs in these three domains in briefer articles, try here, here, and here.
Since Biden is performing well in these domains now, we can assume there has been no meaningful decline from a previously higher level of functioning. There may be a slight fall off in attention, but that’s about all.
Please note: we have now evaluated Biden in all six DSM-5 specified cognitive domains and do not see any significant evidence of decline in any of them. Thus, it certainly appears we can rule out the diagnosis of Neurocognitive Disorder for the president.
We will turn to appraising ex-President Trump’s functioning in the attention, executive functioning, and social cognition domains in Part 2 of this article. But we already have sufficient and relevant data to offer an informed opinion about the president’s and ex-president’s brain health.
Summary and Conclusions
Recently, the country has been discussing the possibility of meaningful cognitive decline with President Biden and ex-President Trump. This concern has been triggered by what many perceive as their periodic struggles with language. Some of this commentary comes from obvious partisan hit jobs, captured by video mashups of the candidate’s most fallible moments. These presentations, quite popular on Fox News and many social media echo chambers, employ the casual use of descriptors such as “senile” and come to facile conclusions that are belied by biased and faulty assumptions. One can only hope they don’t have much impact beyond the political silos within which they reverberate.
Those seeking a more objective assessment of their brain health have been frustrated by the lack of medical information put out by the candidates and the inherent limitations of “diagnosing at a distance”, which is the only resort available when you don’t have their collaboration to undergo a comprehensive neuropsychological examination.
This article describes an effort to elevate the national discussion by (1) injecting a measure of scientific rigor into our observations of Biden’s and Trump’s recent verbal struggles through the use of operationally defined checklists, and (2) subjecting all the relevant information we do have to the guidelines spelled out in DSM-5 concerning the diagnosis of Neurocognitive Disorder. Following these two steps can lead us to an informed opinion on their brain health that is more objective and empirically supported and overcomes some of the limitations involved in “diagnosing at a distance”.
The authors of the Neurocognitive Disorders chapter in DSM-5 (latest revision in 2022) included some of the globe’s leading experts in geriatric psychiatry, neurology, neuropsychology, and psychiatric research. They relied on the latest research to formulate diagnostic criteria for this group of disorders. To arrive at a diagnosis of Neurocognitive Disorder (NCD), DSM-5 stipulates that you need to show a decline in one or more areas of functioning (referred to as cognitive domains): attention, learning and memory, language, perceptual-motor, executive functioning, and social cognition. If you can demonstrate a decline in one of these areas in your patient, then you can strongly consider a diagnosis of either Mild Neurocognitive Disorder or Major Neurocognitive Disorder, depending on whether the decline is “modest” or “significant.” In Mild NCD, struggles with independent living are just beginning to emerge, whereas in Major NCD, there is significant erosion in the capacity for independent living. Mild NCD, with a few exceptions, progresses to Major NCD.
The data to sift for one of these diagnoses for Biden or Trump comes from archival sources (primarily medical records available to the public and videotape that allows for direct behavioral observation) and informant sources (mainly biographies, insider accounts, and profiles by journalists). From these sources, you can begin to make appraisals about a possible decline in all domains, particularly the trait-like domains of executive functioning and social cognition. In the memory, attention, and perceptual-motor domains, we can also make some common-sense judgments from these data sources. However, in these domains, we are limited by the lack of neuropsychological testing that could provide fine-grain assessments to measure possible decline. It should also be noted that in these three domains -in contrast to the executive functioning and social cognition domains — there is typically a slight drop off in functioning as one ages.
There is one domain, language, where we do not need formal testing or collaboration from the candidates. We can make fine-grain assessments of language behavior from speech samples. We can scan speech samples of Biden and Trump for diagnostically relevant verbal markers. These are operationally-defined verbal behaviors that have been linked to neurodegenerative disease. There are voluminous videotaped speech samples of both men from middle age to the present to measure the emergence of these markers.
From all the data we have on hand and relying on the diagnostic criteria of DSM-5, we can put forth the following informed opinions:
1. Based on Biden’s public health records, reports from biographers and insiders, and direct behavioral observation, he does not warrant consideration for a Neurocognitive Disorder at this time in his life. He appears to have a healthy brain, despite whatever struggles he might have with aging. By all accounts, he performs exceptionally well in the executive functioning and social cognition domains.
2. From all the same data sources, and primarily because of the quality of his language struggles, ex-President Trump deserves serious consideration for a diagnosis of Neurocognitive Disorder, a diagnosis which is strongly associated with neurodegenerative disease, a diagnosis which is likely beginning to express itself with suboptimal functioning in a number of areas, and a diagnosis which carries with it a significantly increased risk of progressing to Major Neurocognitive Disorder.
Part Two of this article is available here.
APPENDIX
Diagnostic Criteria for Mild Neurocognitive Disorder
A. Evidence of modest cognitive decline from a previous level of performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual–motor, or social cognition) based on:
1. Concern of the individual, a knowledgeable informant, or the clinician that there has been a mild decline in cognitive function; and
2. A modest impairment in cognitive performance, preferably documented by standardized neuropsychological testing or, in its absence, another quantified clinical assessment.
3. The cognitive deficits do not interfere with capacity for independence in everyday activities (that is, complex instrumental activities of daily living such as paying bills or managing medications are preserved, but greater effort, compensatory strategies, or accommodation may be required).
4. The cognitive deficits do not occur exclusively in the context of a delirium.
5. The cognitive deficits are not better explained by another mental disorder (for example, major depressive disorder or schizophrenia).
Diagnostic Criteria for Major Neurocognitive Disorder
A. Evidence of significant cognitive decline from a previous level of performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual–motor, or social cognition) based on:
1. Concern of the individual, a knowledgeable informant, or the clinician that there has been a significant decline in cognitive function; and
2. A substantial impairment in cognitive performance, preferably documented by standardized neuropsychological testing or, in its absence, another quantified clinical assessment.
B. The cognitive deficits interfere with independence in everyday activities (that is, at a minimum, requiring assistance with complex instrumental activities of daily living such as paying bills or managing medications).
C. The cognitive deficits do not occur exclusively in the context of a delirium.
D. The cognitive deficits are not better explained by another mental disorder.
Specify:
· Without behavioral disturbance: if the cognitive disturbance is not accompanied by any clinically significant behavioral disturbance
· With behavioral disturbance (specify disturbance): if the cognitive disturbance is accompanied by a clinically significant behavioral disturbance (for example, psychotic symptoms, mood disturbance, agitation, apathy, or other behavioral symptoms). For example, major depressive disorder or schizophrenia.
Subtypes with diagnostic criteria in DSM‐5
· Alzheimer disease
· Frontotemporal lobar degeneration
· HIV infection
· Huntington disease
· Lewy body disease
· Parkinson disease
· Prion disease
· Substance and/or medication use
· Traumatic brain injury
· Vascular disease
· Another medical condition
· Multiple etiologies
· Unspecified
Please note: This article is not financed by or related to any political campaign and may not be considered political advertising or action on behalf of any political candidate. All statements and opinions are those of the author alone, including any political endorsements made. The information published in this article is for information only and is not intended to provide psychological therapy or diagnostic advice and/or recommendations to any persons aside from its subjects, Donald J. Trump and Joseph R. Biden, public figures. The content of this article is intended to provide informational, scientific and educational material based on psychological science. The content of this article solely reflects the views and perspectives of its author and does not necessarily reflect the views or positions of the American Psychological Association, medium.com, or any other person and/or entity not otherwise listed as an author.
